

Beyond low-density lipoprotein cholesterol levels: Impact of prior statin treatment on ischemic stroke outcomes
- PMID: 39524491
- PMCID: PMC11550173
- DOI: 10.1016/j.xinn.2024.100713
Beyond low-density lipoprotein cholesterol levels: Impact of prior statin treatment on ischemic stroke outcomes
Abstract
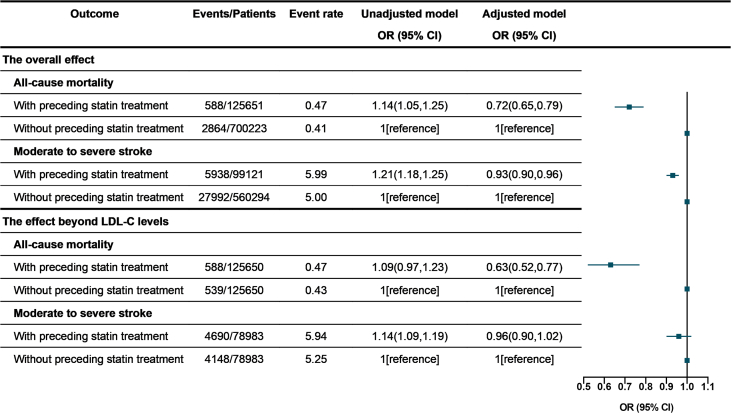
Although essential for cardiovascular therapy, the pleiotropic effects of statins on ischemic stroke lack clinical evidence. This study examined the effects of statins beyond low-density lipoprotein cholesterol (LDL-C) levels on mortality and stroke severity. A total of 825,874 patients with ischemic stroke were included in this study, of whom 125,650 statin users were 1:1 matched with non-users based on their LDL-C levels (±0.05 mmol/L), forming the LDL-C-matched cohort. Associations between preceding statin treatment, in-hospital mortality, and stroke severity (National Institutes of Health Stroke Scale score ≥16) were estimated by multivariate and conditional logistic regression models in overall cohort and LDL-C-matched cohort, respectively. The overall statin effects reduced in-hospital mortality (odds ratio [OR]: 0.72, 95% confidence interval [CI]: 0.65-0.79, p < 0.001) and moderate-to-severe stroke (OR: 0.93, 95% CI: 0.90-0.96, p < 0.001). After matching for LDL-C levels, the reduction in mortality persisted (OR: 0.63, 95% CI: 0.52-0.77, p < 0.001) but not for moderate-to-severe stroke (OR: 0.96, 95% CI: 0.90-1.02, p = 0.215). Stratified by LDL-C levels, the effects of statin beyond LDL-C in reducing mortality remained consistent across all LDL-C ranges but increased with LDL-C reduction for stroke severity and achieved statistical significance at LDL-C <2.60 mmol/L. Mediation analyses showed that LDL-C reduction explained 0.35% (95% CI: 0.23-0.93, p = 0.235) of the statin treatment-mortality relationship and 12.47% (95% CI: 6.78-18.16, p < 0.001) for moderate-to-severe stroke. When examining the overall statin efficacy, LDL-C <2.60 mmol/L was not necessary for mortality reduction but for reducing stroke severity. The efficacy of statins in ischemic stroke outcomes is primarily derived from their effects beyond the LDL-C levels, suggesting that their neuroprotective effects should be considered in addition to their lipid-lowering effects.
© 2024 The Author(s).
Conflict of interest statement
The authors have nothing to declare.
Figures





References
-
- Lee M., Cheng C.Y., Wu Y.L., et al. Association Between Intensity of Low-Density Lipoprotein Cholesterol Reduction With Statin-Based Therapies and Secondary Stroke Prevention: A Meta-analysis of Randomized Clinical Trials. JAMA Neurol. 2022;79(4):349–358. doi: 10.1001/jamaneurol.2021.5578. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
