

Predictors of Device-Related Thrombus After Left Atrial Appendage Occlusion: TED-F2 Score
- PMID: 39525332
- PMCID: PMC11544226
- DOI: 10.1016/j.cjco.2024.05.015
Predictors of Device-Related Thrombus After Left Atrial Appendage Occlusion: TED-F2 Score
Abstract
Background: Left atrial appendage (LAA) occlusion (LAAO) is performed to prevent LAA thrombus in patients with atrial fibrillation (AF). The risk of device-related thrombus (DRT) on the atrial side of the LAAO device is approximately 4%. Identifying patients at high risk of DRT would enable closer surveillance and more-aggressive anticoagulation to prevent post-LAAO DRT-related stroke.
Methods: From the LAAO registry at The University of Kansas Medical Center, we identified patients who developed DRT. We chose 3 unmatched controls per DRT case from LAAO recipients without DRT. Predictor variables were obtained from transesophageal echocardiogram reports and/or images, transthoracic echocardiogram reports, and chart review. Implant depth was measured from the limbus of the left atrial ridge to the centre of the atrial aspect of the LAAO device, on a 45° transesophageal echocardiogram view.
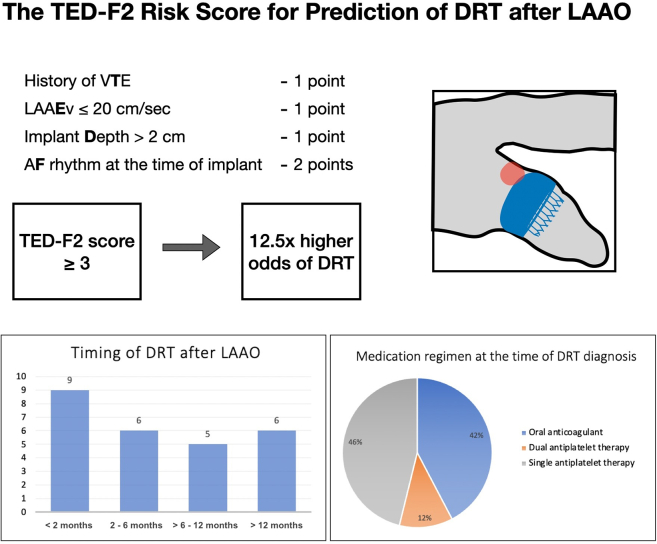
Results: We identified 26 patients with DRT (aged 77.7 ± 9.7 years; 34.6% female) and selected 78 unmatched controls without DRT. Univariate predictors of DRT, comprising a novel TED-F2 score, included history of venous Thromboembolism (23.1% vs 5.1%, P = 0.01), an LAA Emptying velocity ≤ 20 cm/s (45.8% vs 18.9%, P = 0.01), an implant Depth > 2 cm (34.6% vs 12.8%, P = 0.02), and presence of AF rhythm at time of device implantation (50.0 % vs 11.5%, P = 0.0001). A TED-F2 score of ≥ 3 was very strongly associated with DRT-odds ratio 12.5 (95% confidence interval, 3.8-41.1, P < 0.0001).
Conclusions: We propose a novel risk score to predict development of DRT after LAAO, comprising history of venous Thromboembolism, LAA Emptying velocity ≤ 20 cm/s, implant Depth > 2 cm (1 point each), and an AF rhythm at implantation (2 points). A TED-F2 risk score of ≥ 3 identified patients who are at greatly elevated risk of developing DRT.
Résumé: La fermeture de l’appendice auriculaire gauche (AAG) sert à prévenir la formation d’un thrombus à l’AAG en présence d’une fibrillation auriculaire (FA). Le risque de formation de thrombus du côté auriculaire du dispositif de fermeture de l’AAG est d'environ 4 %. La capacité de déterminer quels patients présentent un risque élevé de formation de thrombus liée au dispositif permettrait une surveillance plus étroite et l’administration d’un traitement anticoagulant plus intense pour prévenir un AVC découlant d’un thrombus formé après l’installation d’un dispositif de fermeture de l’AAG.
Méthodologie: Dans le registre des fermetures de l’AAG du centre médical de l’Université du Kansas (University of Kansas Medical Center), nous avons recensé des patients chez qui un thrombus lié à un dispositif s’était formé. Nous avons choisi au hasard 3 fois plus de patients témoins qui avaient subi une fermeture de l’AAG sans qu’un thrombus lié au dispositif se soit formé. Des variables descriptives ont été obtenues à partir de rapports et/ou d’images d’échocardiogrammes transœsophagiens, de rapports d’échocardiogrammes transthoraciques et d’analyses de dossiers. La profondeur de l’implant était mesurée du limbe de la crête auriculaire gauche au centre du côté auriculaire du dispositif de fermeture de l’AAG, sur une vue échocardiographique transœsophagienne à 45°.
Résultats: Nous avons recensé 26 patients (âgés de 77,7 ± 9,7 ans; 34,6 % de femmes) présentant un thrombus lié au dispositif et nous avons sélectionné 78 témoins non appariés sans thrombus lié au dispositif. Les facteurs prédictifs à variable unique du thrombus lié au dispositif, dont un nouveau score TED-F2, comprenaient les antécédents de thromboembolie veineuse (23,1 % vs 5,1 %, p = 0,01), une vitesse de vidange de l’AAG ≤ 20 cm/s (45,8 % vs 18,9 %, p = 0,01), une profondeur de l’implant > 2 cm (34,6 % vs 12,8 %, p = 0,02) et présence d'un rythme de fibrillation auriculaire au moment de l’implantation (50,0 % vs 11,5 %, p = 0,0001). Un score TED-F2 ≥ 3 était fortement corrélé à la formation d’un thrombus lié au dispositif — rapport de cotes de 12,5 (intervalle de confiance à 95 %, 3,8-41,1; p < 0,0001).
Conclusions: Nous proposons un nouveau score de risque pour prédire la formation d’un thrombus lié au dispositif après la fermeture de l’AAG, comprenant des antécédents de thromboembolie veineuse, une vitesse de vidange de l’AAG ≤ 20 cm/s, une profondeur de l’implant > 2 cm (1 point chacun) et un rythme de fibrillation auriculaire à l’implantation (2 points). Un score de risque TED-F2 ≥ 3 indiquait un risque très élevé de formation de thrombus lié au dispositif.
© 2024 The Authors.
Figures

References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., et al. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147:e93–e621. - PubMed
-
- Blackshear J.L., Odell J.A. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg. 1996;61:755–759. - PubMed
-
- Hart R.G., Pearce L.A., Aguilar M.I. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
-
- Saw J., Holmes D.R., Cavalcante J.L., et al. SCAI/HRS expert consensus statement on transcatheter left atrial appendage closure. Heart Rhythm. 2023;20:e1–e16. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
