

Intra-atrial block after COVID-19 vaccination-induced fulminant myocarditis: a case report
- PMID: 39525510
- PMCID: PMC11549679
- DOI: 10.1093/ehjcr/ytae580
Intra-atrial block after COVID-19 vaccination-induced fulminant myocarditis: a case report
Abstract
Background: Myocarditis is associated with an increased risk of conduction disturbances during the acute phase, which recovers in most cases but rarely recurs during the chronic phase.
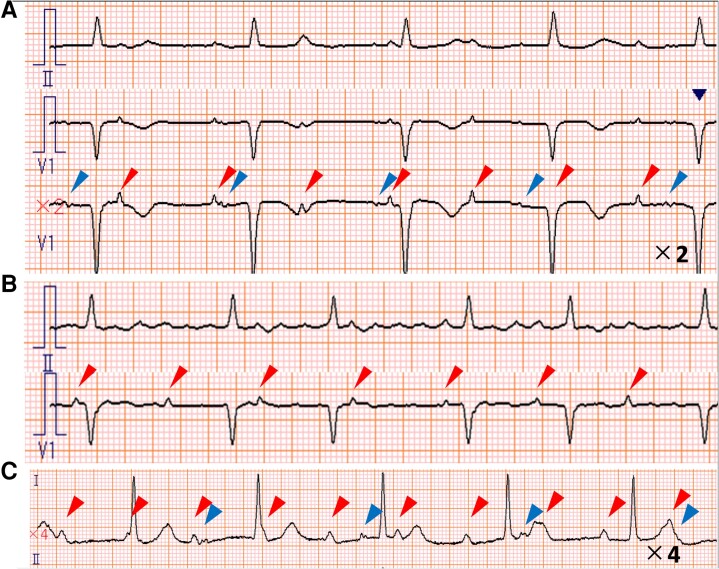
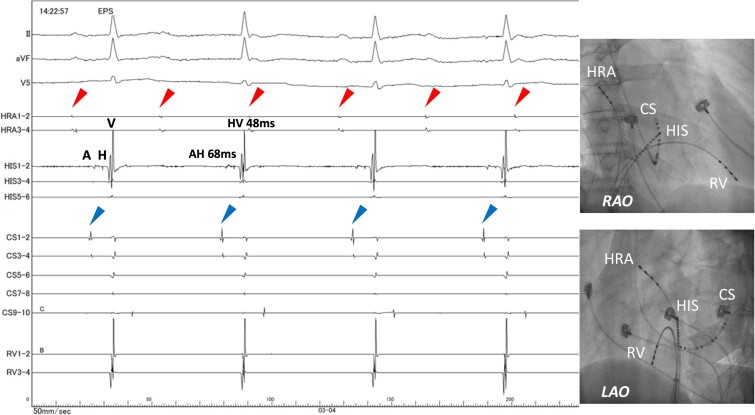
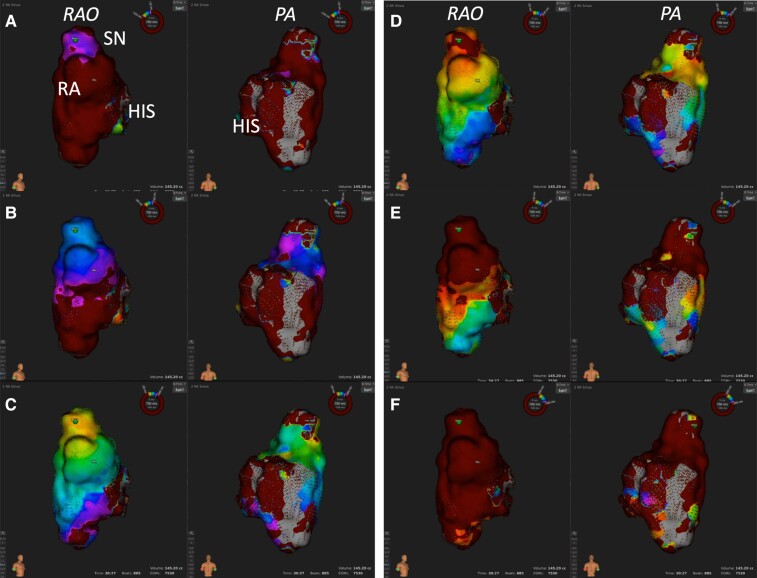
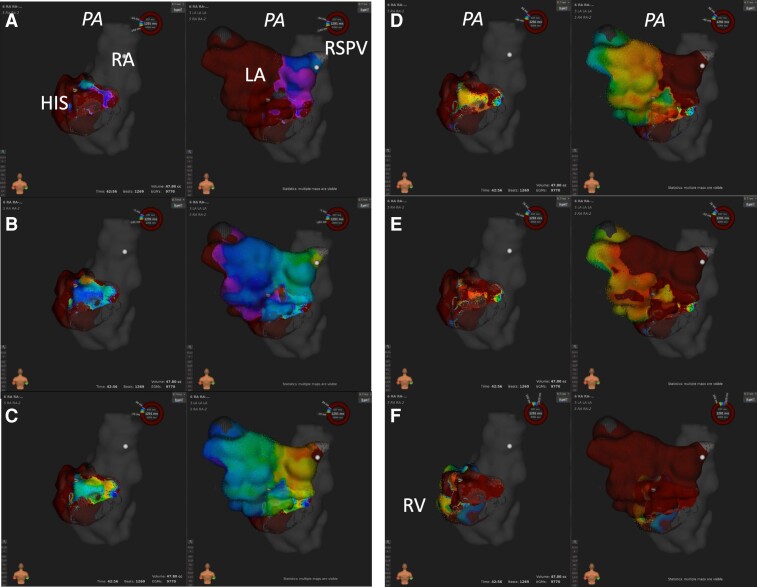
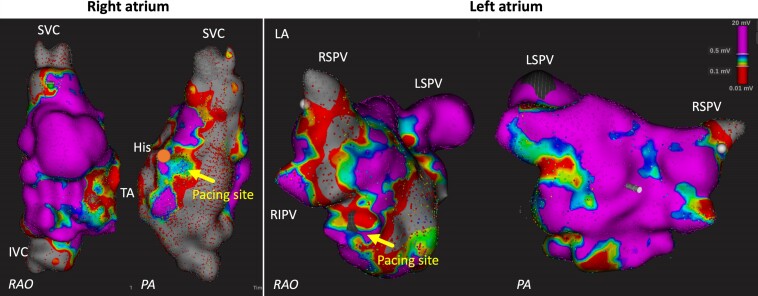
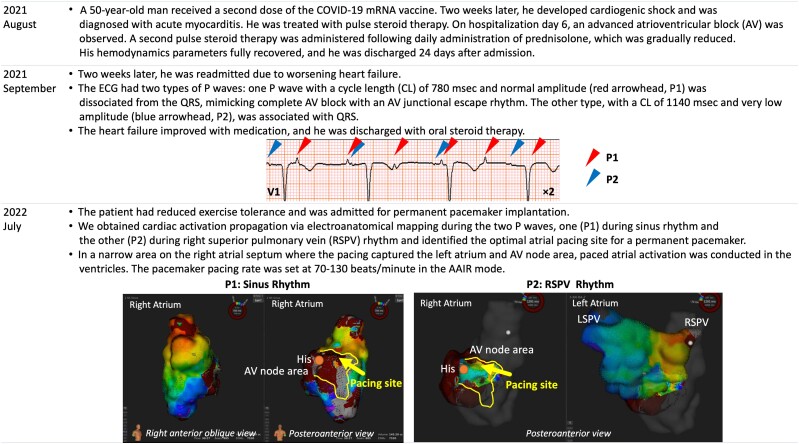
Case summary: A 50-year-old man who developed fulminant myocarditis after COVID-19 mRNA vaccination was discharged 24 days after admission. He was readmitted for heart failure associated with two P waves: one P wave (P1) had a normal amplitude and was dissociated from the QRS, and the other (P2) had a very low amplitude and was associated with the QRS. The patient was referred for pacemaker implantation. Before implantation, an electrophysiological study was conducted using electro-anatomical mapping (EAM). During the P1 wave activation, the sinus rhythm spread to the right atrium but was blocked in the atrioventricular (AV) node area. During P2 activation, the activation originated from the right superior pulmonary vein (RSPV), spread to the left atrium and AV node area through the interatrial septum, and was conducted to the right ventricle, exhibiting a complete intra-atrial block with two discrete rhythms. An atrial lead was successfully placed in a narrow area in the right atrial septum where the pacing captured the left atrium and AV node area under the guidance of EAM findings.
Discussion: The EAM technology has demonstrated intra-atrial block and two types of atrial rhythms, sinus and RSPV. Electro-anatomical mapping findings were also useful for identifying the ideal pacemaker implantation site. Synchrony between the left atrium and ventricle via His-Purkinje conduction, which was achieved with EAM-guided atrial septal pacing, was prioritized.
Keywords: COVID-19 mRNA vaccine; Case report; Intra-atrial block; Myocarditis; Pacemaker; Two P waves.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Similar articles
-
Optimal site of pacemaker lead implantation for persistent atrial standstill guided by electroanatomical mapping following a cox-maze procedure: a case report.Eur Heart J Case Rep. 2024 Dec 2;8(12):ytae647. doi: 10.1093/ehjcr/ytae647. eCollection 2024 Dec. Eur Heart J Case Rep. 2024. PMID: 39687540 Free PMC article.
-
Biventricular pacing (cardiac resynchronization therapy): an evidence-based analysis.Ont Health Technol Assess Ser. 2005;5(13):1-60. Epub 2005 Sep 1. Ont Health Technol Assess Ser. 2005. PMID: 23074464 Free PMC article.
-
Atrial septal pacing to synchronize atrial depolarization in patients with delayed interatrial conduction.Pacing Clin Electrophysiol. 1998 Nov;21(11 Pt 2):2220-5. doi: 10.1111/j.1540-8159.1998.tb01156.x. Pacing Clin Electrophysiol. 1998. PMID: 9825322
-
Hybrid therapy of atrial fibrillation.Ital Heart J. 2002 Oct;3(10):571-8. Ital Heart J. 2002. PMID: 12478814 Review.
-
Morphology and electrophysiology of the mammalian atrioventricular node.Physiol Rev. 1988 Apr;68(2):608-47. doi: 10.1152/physrev.1988.68.2.608. Physiol Rev. 1988. PMID: 2451833 Review.
References
-
- Peretto G, Sala S, Rizzo S, De Luca G, Campochiaro C, Sartorelli S, et al. Arrhythmias in myocarditis: state of the art. Heart Rhythm 2019;16:793–801. - PubMed
-
- Ogunbayo GO, Elayi SC, Ha LD, Olorunfemi O, Elbadawi A, Saheed D, et al. Outcomes of heart block in myocarditis: a review of 31,760 patients. Heart Lung Circ 2019;28:272–276. - PubMed
Publication types
LinkOut - more resources
Full Text Sources