

Disparities in casemix, acute interventions, discharge destinations and mortality of patients with traumatic brain injury between Europe and India
- PMID: 39526450
- PMCID: PMC11614187
- DOI: 10.7189/jogh.14.04227
Disparities in casemix, acute interventions, discharge destinations and mortality of patients with traumatic brain injury between Europe and India
Abstract
Background: Traumatic brain injury (TBI) is a major global health problem that disproportionally affects low- and middle-income countries. The needs for patients with TBI therefore may differ between levels of national development. We aimed to describe differences in epidemiology and acute care provision of TBI between India and Europe.
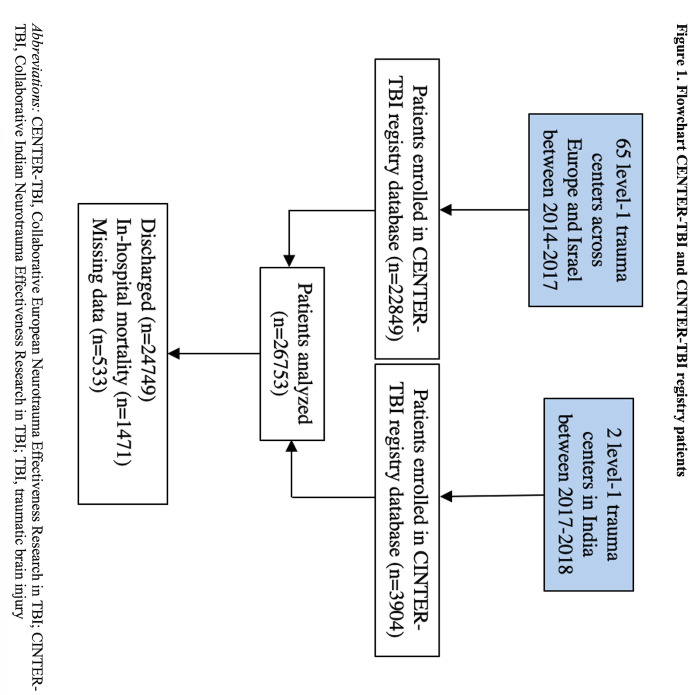
Methods: We used data from two prospective observational registry studies - the Collaborative Indian NeuroTrauma Effectiveness Research in TBI (CINTER-TBI) and the Collaborative European NeuroTrauma Effectiveness Research in TBI (CENTER-TBI), which included TBI patients with an indication for brain CT-scan presenting to 65 centres across Europe and Israel and two trauma centres in India. We performed descriptive analyses of demographic, injury, and treatment characteristics and used random-effects logistic regression with covariate adjustment to examine the likelihood of acute neurosurgical interventions and in-hospital mortality.
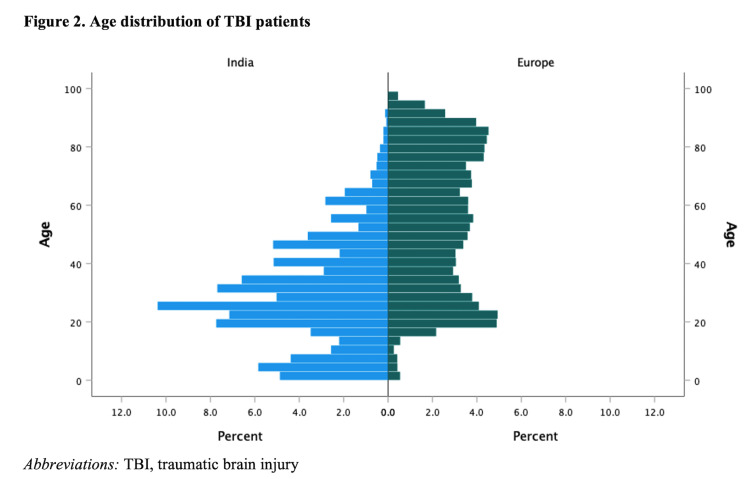
Results: We included 22 849 patients from CENTER-TBI and 3904 from CINTER-TBI. The median age in Europe was 55 years (IQR = 32-76) compared to 27 years (IQR = 18-40) in India. The most common cause of TBI in Europe were falls (n = 12150 (53%), while traffic incidents predominated in India (n = 2130 (55%)). The proportion of patients with severe TBI was higher in India (n = 867 (22%)) than in Europe (n = 1661 (7%). Professional pre-hospital care involving ambulance service was utilised by three-fourths (n = 17203 (75%)) of European and less than a one-tenth (n = 224 (6%)) of Indian patients in our sample. Patients with severe TBI were more likely to undergo surgical contusion/haematoma evacuation in India compared to Europe (OR = 2.0; 95% CI = 1.7-2.5) and Indian patients had higher odds of undergoing intracranial pressure monitor placement (OR = 2.3; 95% CI = 2.0-2.7). A primary decompressive craniectomy was likewise more often performed in the Indian cohort (OR = 5.1; 95% CI = 3.5-7.5). Discharge destinations in Europe included rehabilitation centres (n = 1261 (6%)) or nursing homes (n = 1208 (5%)), which was rarely the case in India (n = 13 (0%) and n = 9 (0%), respectively).
Conclusions: Substantial disparities between India and Europe exist along the neurotrauma care chain, with both systems being likely to face unique features and challenges in the future.
Copyright © 2024 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Figures
References
-
- Singh M, Pal R, Yarasani P, Bhandarkar P, Munivenkatappa A, Agrawal A.International Classification of Diseases-Based Audit of the Injury Database to Understand the Injury Distribution in Patients Who have Sustained a Head Injury (International Classification of Diseases Codes: S00-S09). J Emerg Trauma Shock. 2018;11:253–64. 10.4103/JETS.JETS_90_17 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
