

Indirect comparison of deucravacitinib and other systemic treatments for moderate to severe plaque psoriasis in Asian populations: A systematic literature review and network meta-analysis
- PMID: 39526612
- PMCID: PMC11624152
- DOI: 10.1111/1346-8138.17448
Indirect comparison of deucravacitinib and other systemic treatments for moderate to severe plaque psoriasis in Asian populations: A systematic literature review and network meta-analysis
Abstract
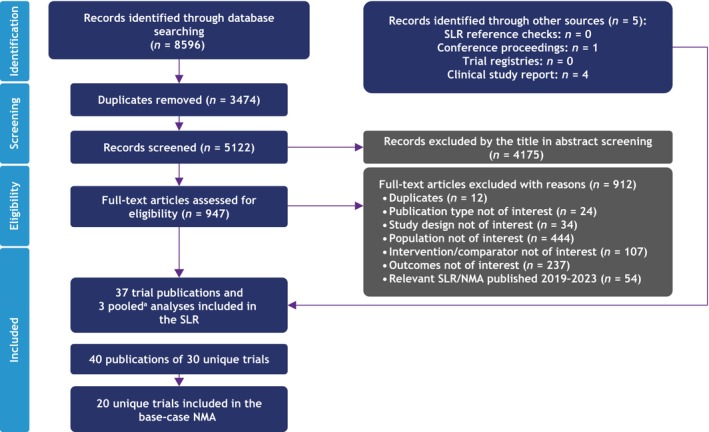
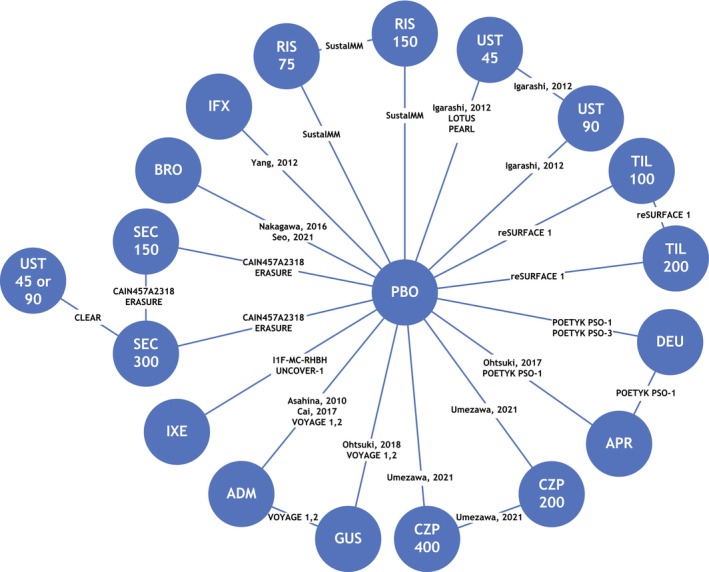
Expanding the systemic treatment options for patients with psoriasis, deucravacitinib, an oral, selective, allosteric tyrosine kinase 2 inhibitor is approved in the United States, European Union, China, Japan, Taiwan, Korea, and other countries for the treatment of adults with moderate to severe plaque psoriasis who are candidates for systemic therapy. Evidence suggests the comparative efficacy of systemic therapies may be different in Asian versus White patients. This systematic review and network meta-analysis (NMA) evaluated the clinical efficacy associated with deucravacitinib and other biologic or non-biologic systemic treatments for moderate to severe plaque psoriasis in Asian populations. Electronic databases were searched to identify randomized trials of the interventions of interest. Multinomial random effects models adjusting for baseline placebo risk were used to estimate Psoriasis Area and Severity Index (PASI) responses at weeks 10-16. Of 8596 studies identified, 20 were included in the NMA. The estimated PASI 75 and 90 (95% credible interval) response rates for deucravacitinib were estimated to be 66% (49%-80%) and 40% (24%-58%) in Asian populations, notably higher than placebo (6% [4%-9%] and 1% [0.8-2%]) and apremilast (24% [12%-40%] and 9% [4%-20%]). No statistically significant difference was observed in PASI 75 and 90 responses between deucravacitinib and adalimumab, certolizumab pegol, infliximab, ustekinumab, and tildrakizumab. Deucravacitinib demonstrated robust efficacy in the Asian population, with PASI 75 and 90 responses comparable to some biologics. Deucravacitinib provides a convenient oral therapy with efficacy similar to several biologic therapies.
Keywords: Apremilast; biologics; deucravacitinib; network meta‐analysis; psoriasis.
© 2024 The Author(s). The Journal of Dermatology published by John Wiley & Sons Australia, Ltd on behalf of Japanese Dermatological Association.
Conflict of interest statement
Tsen‐Fang Tsai has served as a clinical trial investigator or consultant with honoraria from AbbVie, AnaptysBio, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Galderma, GSK, Janssen‐Cilag, Leo Pharma, Lilly, Merck, Novartis, Pfizer, PharmaEssentia, Sanofi, Sun Pharma, and UCB. Yayoi Tada has received research grants from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eisai, Jimro, Kyowa Kirin, Leo Pharma, Lilly, Maruho, Sun Pharma, Taiho Pharmaceutical, Tanabe‐Mitsubishi, Torii Pharmaceutical, and UCB; and honoraria from AbbVie, Amgen, Boehringer Ingelheim, Bristol Myers Squibb, Eisai, Janssen, Jimro, Kyowa Kirin, Leo Pharma, Lilly, Maruho, Novartis, Pfizer, Sun Pharma, Taiho Pharmaceutical, Tanabe‐Mitsubishi, Torii Pharmaceutical, and UCB; and consulting fees from AbbVie, Boehringer Ingelheim, Bristol Myers Squibb, Janssen, Lilly, Maruho, Novartis, Taiho Pharmaceutical, and UCB; Dr. Tada was not associated with the editorial process of this manuscript. Camy Kung, Yichen Zhong, Renata M. Kisa are employees and shareholders of Bristol Myers Squibb. Allie Cichewicz, Katarzyna Borkowska, and Tracy Westley are employees of Evidera, which received funding from Bristol Myers Squibb. Yu‐Huei Huang served as a clinical trial investigator or received honoraria as a consultant and speaker for AbbVie, Bristol Myers Squibb, Celgene, Janssen‐Cilag, Novartis, and Pfizer. Xing‐Hua Gao served as a consultant for AbbVie, AstraZeneca, Boehringer Ingelheim, GSK, Janssen Xian, Lilly, and Novartis. Seong‐Jin Jo served as a clinical trial investigator, advisory board member, consultant, or received research grants or speaker's honoraria from AbbVie, Boehringer Ingelheim, Bristol Myers Squibb, Celltrion Healthcare, Daewoong, Green Cross Laboratories, Janssen, Kolon Pharma, Leo Pharma, Lilly, Novartis, Pfizer, Sanofi, UCB, and Yuhan. April W. Armstrong served as a research investigator, scientific advisor, and/or speaker for AbbVie, Almirall, Arcutis, Aslan Pharmaceuticals, Beiersdorf, Boehringer Ingelheim, Bristol Myers Squibb, Dermavant, Dermira, EPI Health, Incyte, Janssen, Leo Pharma, Lilly, Mindera Health, Nimbus, Novartis, Ortho Dermatologics, Pfizer, Regeneron, Sanofi, Sun Pharma, and UCB.
Figures



References
-
- Sotyktu [package insert]. Princeton, NJ: Bristol Myers Squibb; 2022.
-
- Sotyktu [package insert]. Tokyo, Japan: Bristol Myers Squibb K.K; 2022.
-
- Sotyktu [summary of product characteristics]. Dublin, Ireland: Bristol Myers Squibb Pharmaceutical Operations; 2023.
-
- Strober B, Thaçi D, Sofen H, Kircik L, Gordon KB, Foley P, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52‐week, randomized, double‐blinded, Program fOr Evaluation of TYK2 inhibitor psoriasis second phase 3 trial. J Am Acad Dermatol. 2023;88:40–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
