

Derivation and internal validation of prediction models for pulmonary hypertension risk assessment in a cohort inhabiting Tibet, China
- PMID: 39526735
- PMCID: PMC11554304
- DOI: 10.7554/eLife.98169
Derivation and internal validation of prediction models for pulmonary hypertension risk assessment in a cohort inhabiting Tibet, China
Abstract
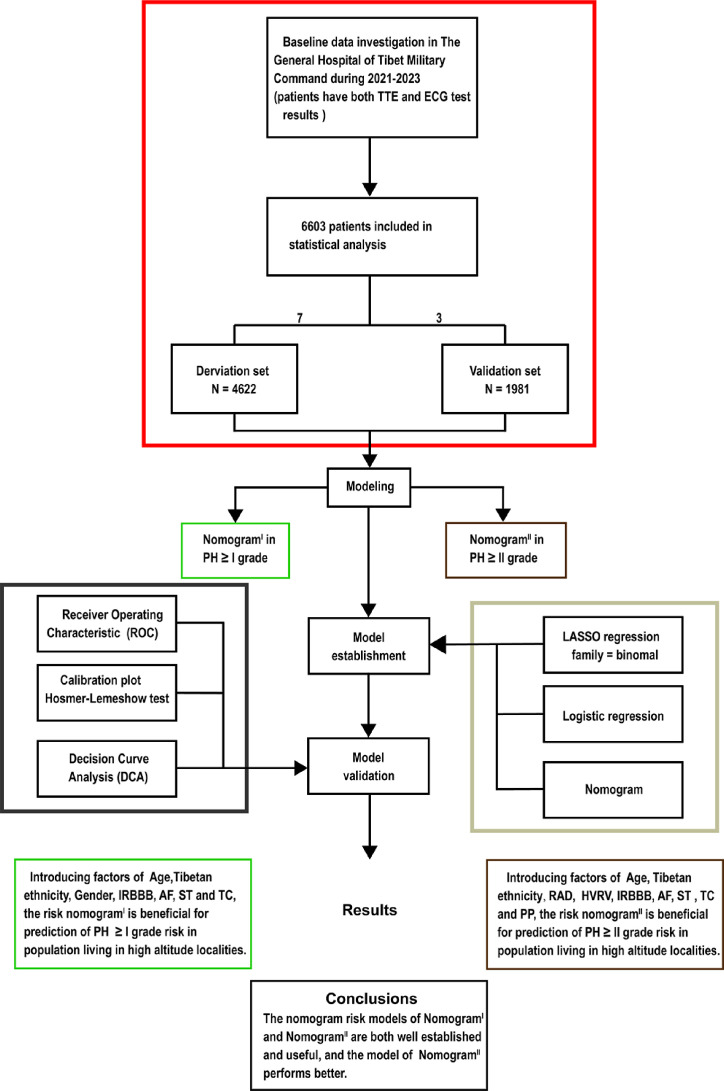
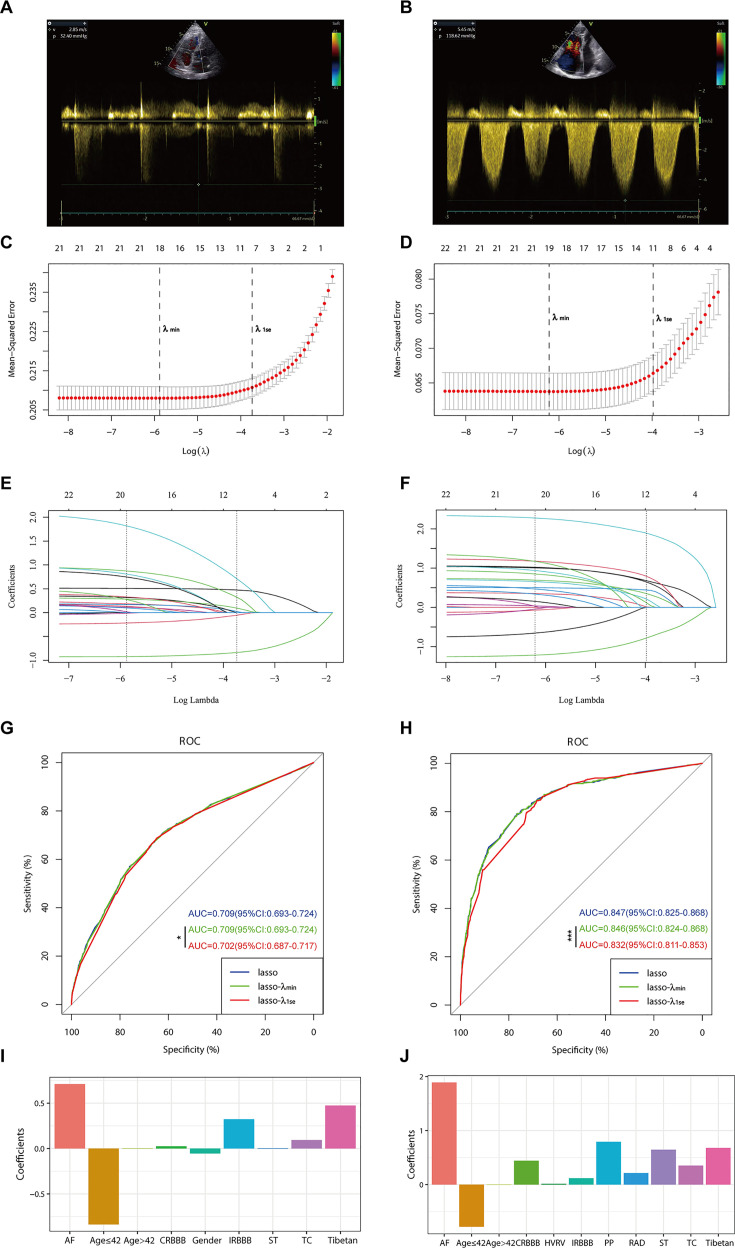
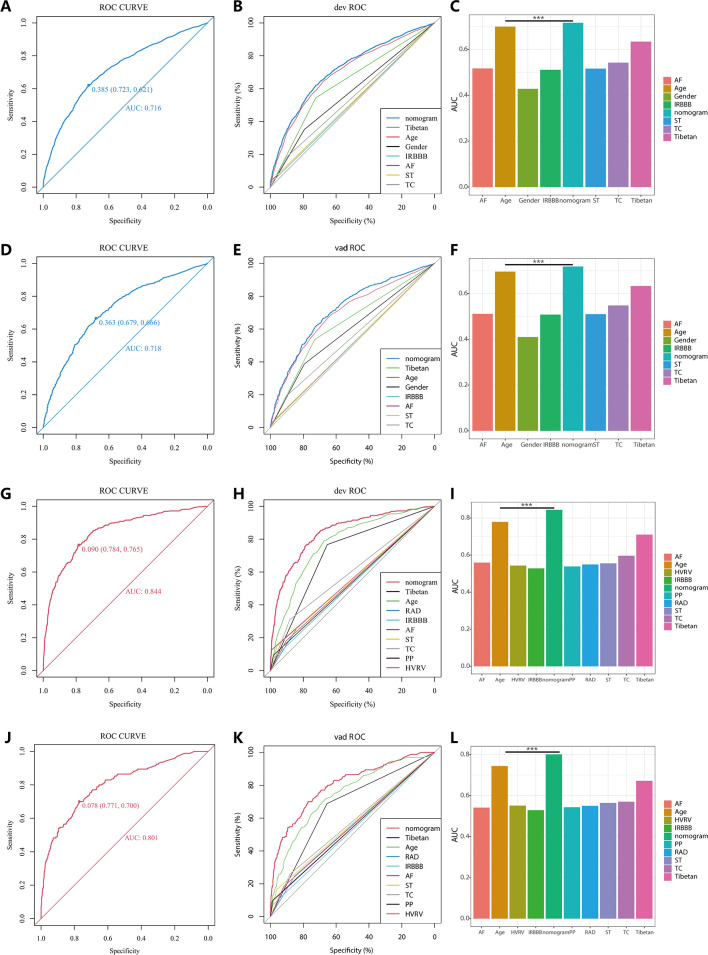
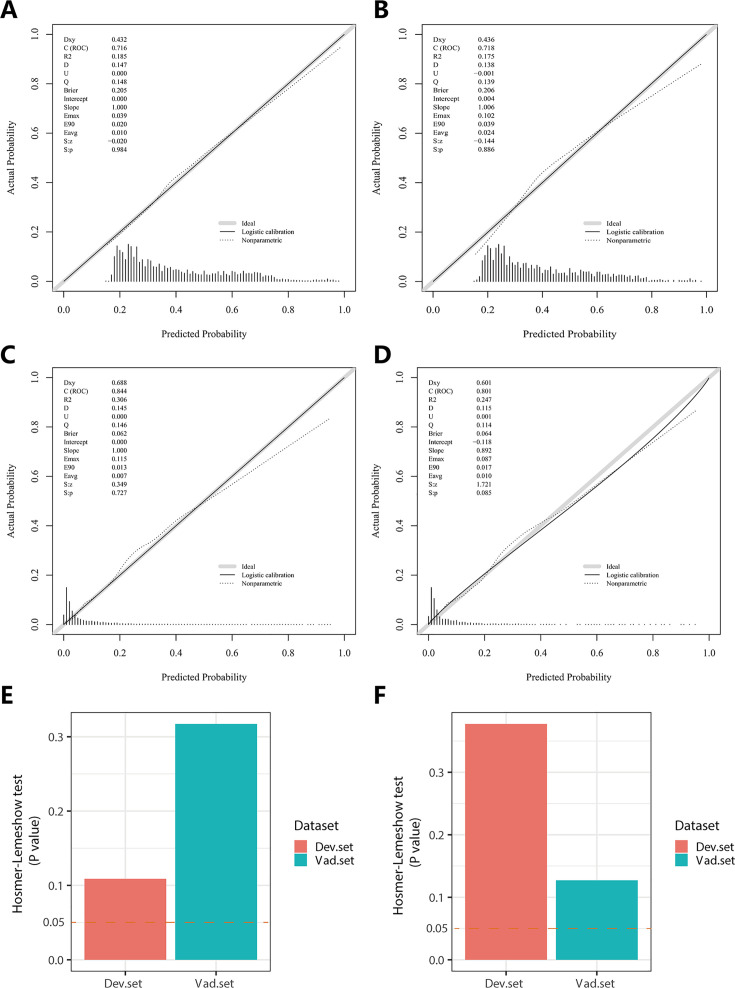
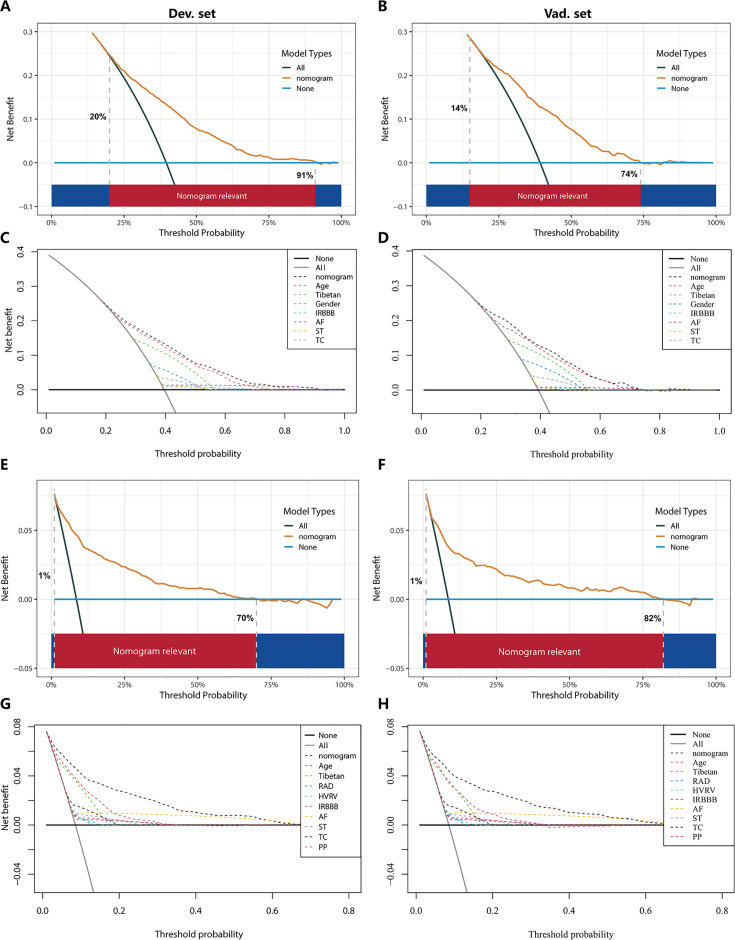
Individuals residing in plateau regions are susceptible to pulmonary hypertension (PH) and there is an urgent need for a prediction nomogram to assess the risk of PH in this population. A total of 6603 subjects were randomly divided into a derivation set and a validation set at a ratio of 7:3. Optimal predictive features were identified through the least absolute shrinkage and selection operator regression technique, and nomograms were constructed using multivariate logistic regression. The performance of these nomograms was evaluated and validated using the area under the curve (AUC), calibration curves, the Hosmer-Lemeshow test, and decision curve analysis. Comparisons between nomograms were conducted using the net reclassification improvement (NRI) and integrated discrimination improvement (IDI) indices. NomogramI was established based on independent risk factors, including gender, Tibetan ethnicity, age, incomplete right bundle branch block (IRBBB), atrial fibrillation (AF), sinus tachycardia (ST), and T wave changes (TC). The AUCs for NomogramI were 0.716 in the derivation set and 0.718 in the validation set. NomogramII was established based on independent risk factors, including Tibetan ethnicity, age, right axis deviation, high voltage in the right ventricle, IRBBB, AF, pulmonary P waves, ST, and TC. The AUCs for NomogramII were 0.844 in the derivation set and 0.801 in the validation set. Both nomograms demonstrated satisfactory clinical consistency. The IDI and NRI indices confirmed that NomogramII outperformed NomogramI. Therefore, the online dynamic NomogramII was established to predict the risks of PH in the plateau population.
Keywords: computational biology; electrocardiogram; high altitude; human; nomogram; prediction model; pulmonary hypertension; systems biology; transthoracic echocardiography.
© 2024, Tang, Yang et al.
Conflict of interest statement
JT, RY, HL, XW, ZY, WC, YJ, GZ, LM, YX No competing interests declared
Figures

Update of
- doi: 10.1101/2024.04.29.24306542
- doi: 10.7554/eLife.98169.1
- doi: 10.7554/eLife.98169.2
Similar articles
-
Development and validation of a nomogram to better predict hypertension based on a 10-year retrospective cohort study in China.Elife. 2021 May 28;10:e66419. doi: 10.7554/eLife.66419. Elife. 2021. PMID: 34047697 Free PMC article.
-
A nomogram integrating non-ECG factors with ECG to screen left ventricular hypertrophy among hypertensive patients from northern China.J Hypertens. 2022 Feb 1;40(2):264-273. doi: 10.1097/HJH.0000000000003003. J Hypertens. 2022. PMID: 34992197
-
Development and validation of a nomogram model for prolonged length of stay in spinal fusion patients: a retrospective analysis.BMC Med Inform Decis Mak. 2024 Dec 5;24(1):373. doi: 10.1186/s12911-024-02787-7. BMC Med Inform Decis Mak. 2024. PMID: 39639314 Free PMC article.
-
Development and validation of a nomogram for predicting in-hospital mortality of patients with cervical spine fractures without spinal cord injury.Eur J Med Res. 2024 Jan 29;29(1):80. doi: 10.1186/s40001-024-01655-4. Eur J Med Res. 2024. PMID: 38287435 Free PMC article.
-
Clinical characteristics and a diagnostic model for high-altitude pulmonary edema in habitual low altitude dwellers.PeerJ. 2024 Sep 26;12:e18084. doi: 10.7717/peerj.18084. eCollection 2024. PeerJ. 2024. PMID: 39346082 Free PMC article.
References
-
- Benza RL, Miller DP, Gomberg-Maitland M, Frantz RP, Foreman AJ, Coffey CS, Frost A, Barst RJ, Badesch DB, Elliott CG, Liou TG, McGoon MD. Predicting survival in pulmonary arterial hypertension: insights from the registry to evaluate early and long-term pulmonary arterial hypertension disease management (REVEAL) Circulation. 2010;122:164–172. doi: 10.1161/CIRCULATIONAHA.109.898122. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
