

Acute and chronic hypopituitarism following traumatic brain injury: a systematic review and meta-analysis
- PMID: 39527353
- PMCID: PMC11554839
- DOI: 10.1007/s10143-024-03088-3
Acute and chronic hypopituitarism following traumatic brain injury: a systematic review and meta-analysis
Abstract
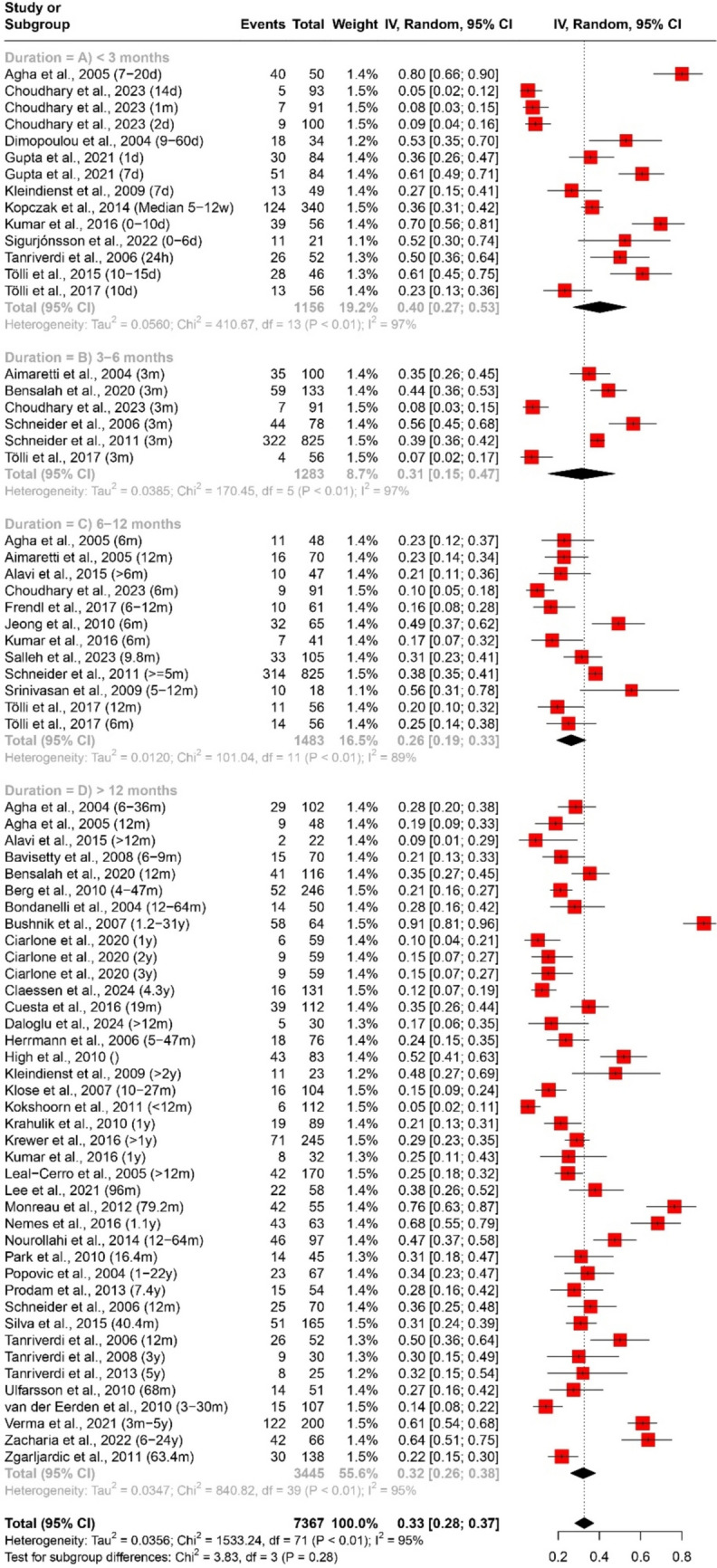
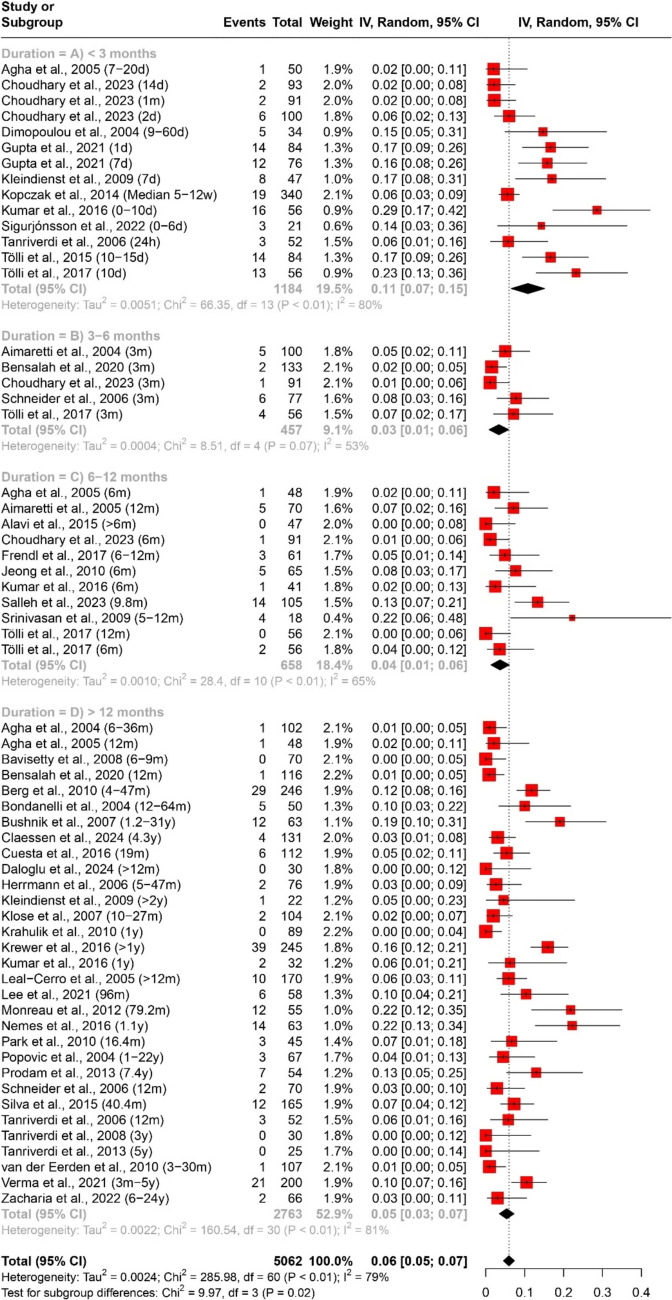
Traumatic brain injury (TBI) is associated with various endocrine abnormalities, including pituitary axis dysfunction. Understanding the prevalence and temporal patterns of these dysfunctions is crucial for effective clinical management. This study aimed to systematically review the literature and conduct a meta-analysis to determine the prevalence of pituitary axis dysfunction following TBI, assess temporal patterns across different post-injury durations, and identify potential contributing factors. A comprehensive search was conducted across multiple electronic databases between 1st of January 2000 until 31st March 2024. Studies reporting the prevalence of pituitary axis dysfunction post-TBI were included. Pooled estimates with 95% confidence intervals (CIs) were calculated using random-effects models in the R statistical software. Subgroup analyses were performed based on duration post-TBI (< 3 months, 3-6 months, 6-12 months, > 12 months) to explore temporal variations. Heterogeneity was assessed using the I^2 statistic. A total of 52 studies were included in the meta-analysis, encompassing 7367 participants. The pooled estimate for the prevalence of any pituitary axis dysfunction post-TBI was 33% (95% CI [28%; 37%]). Subgroup analysis by duration revealed varying prevalence rates: < 3 months (40%, 95% CI [27%; 53%]), 3-6 months (31%, 95% CI [15%; 47%]), 6-12 months (26%, 95% CI [19%; 33%]), and > 12 months (32%, 95% CI [26%; 38%]). Prevalence of multiple axes affection was 7% (95% CI [6%; 9%]), with varying rates across durations. Specific axes affection varied: Growth Hormone (GH) deficiency was 18% (95% CI [14%; 21%]), adrenocorticotropic hormone (ACTH) deficiency was 10% (95% CI [8%; 13%]), pituitary-gonadal axis hormones deficiency was 16% (95% CI [12%; 19%]), and thyroid-stimulating hormone (TSH) deficiency was 6% (95% CI [5%; 7%]). This meta-analysis highlights a significant prevalence of pituitary axis dysfunction following TBI, with temporal variations observed across different post-injury durations. The findings underscore the importance of tailored clinical management strategies based on the duration and type of dysfunction. Further research addressing potential contributing factors is warranted to enhance understanding and management of these conditions.
Keywords: Endocrine abnormalities; Meta-analysis; Pituitary axis dysfunction; Prevalence; Temporal patterns; Traumatic brain injury.
© 2024. The Author(s).
Conflict of interest statement
Figures





References
-
- Faul M, Coronado V (2015) Epidemiology of traumatic brain injury. Handb Clin Neurol 127:3–13 - PubMed
-
- Williamson C, Rajajee V (2023) Traumatic brain injury: epidemiology, classification, and pathophysiology. In: Post TW (ed) UpToDate. UpToDate, Waltham
-
- Capizzi A, Woo J, Verduzco-Gutierrez M (2020) Traumatic brain injury: an overview of epidemiology, pathophysiology, and medical management. Med Clin 104(2):213–238 - PubMed
-
- Bonow RH, Barber J, Temkin NR, Videtta W, Rondina C, Petroni G, Lujan S, Alanis V, La Fuente G, Lavadenz A, Merida R, Jibaja M, Gonzáles L, Falcao A, Romero R, Dikmen S, Pridgeon J, Chesnut RM, Global Neurotrauma Research Group (2018) The outcome of severe traumatic brain injury in Latin America. World Neurosurg 111:e82–e90. 10.1016/j.wneu.2017.11.171 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
