

A model of lymphocryptovirus-associated post-transplant lymphoproliferative disorder in immunosuppressed Mauritian cynomolgus macaques
- PMID: 39527641
- PMCID: PMC11581395
- DOI: 10.1371/journal.ppat.1012644
A model of lymphocryptovirus-associated post-transplant lymphoproliferative disorder in immunosuppressed Mauritian cynomolgus macaques
Abstract
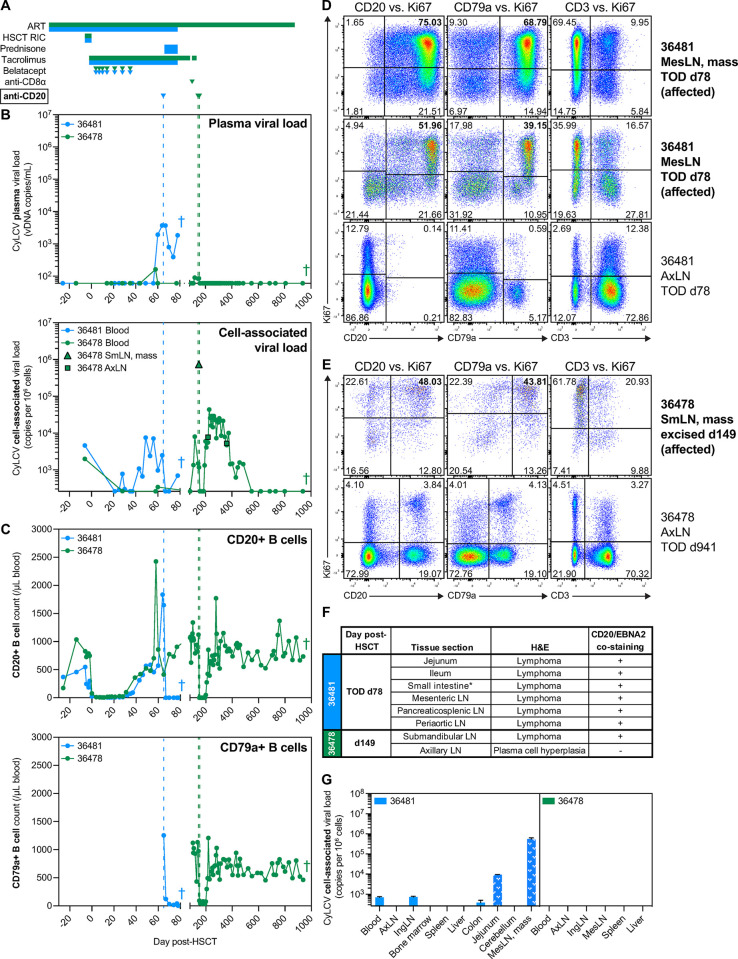
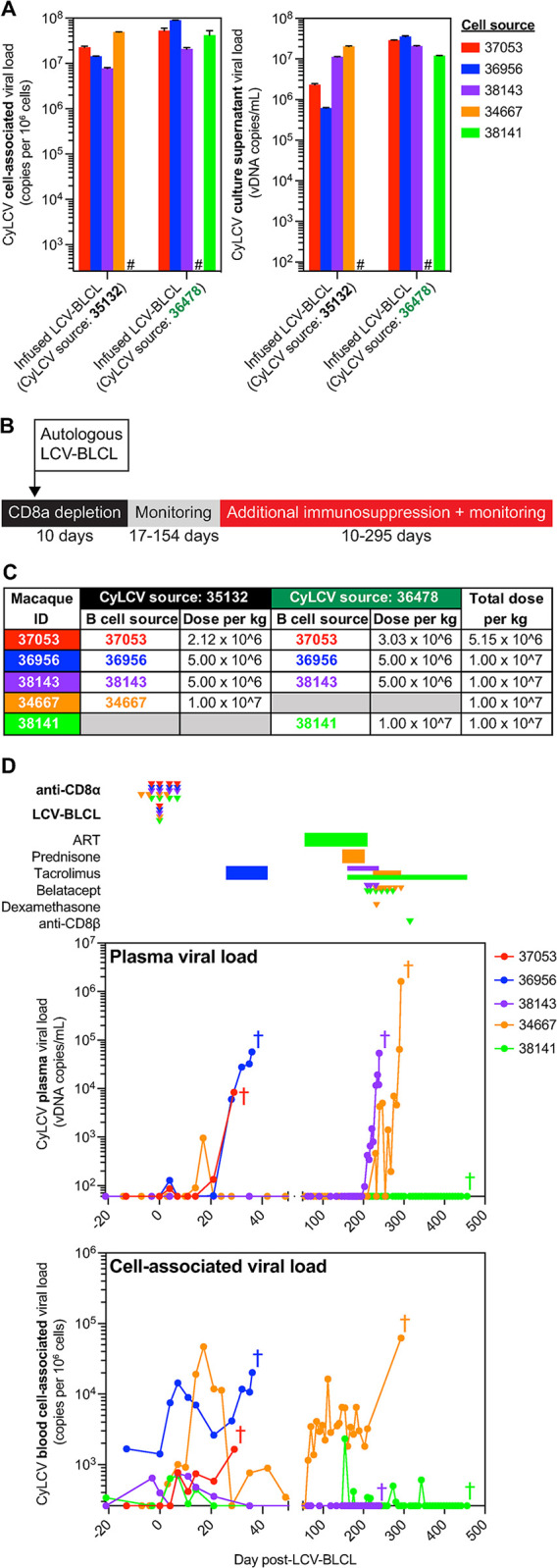
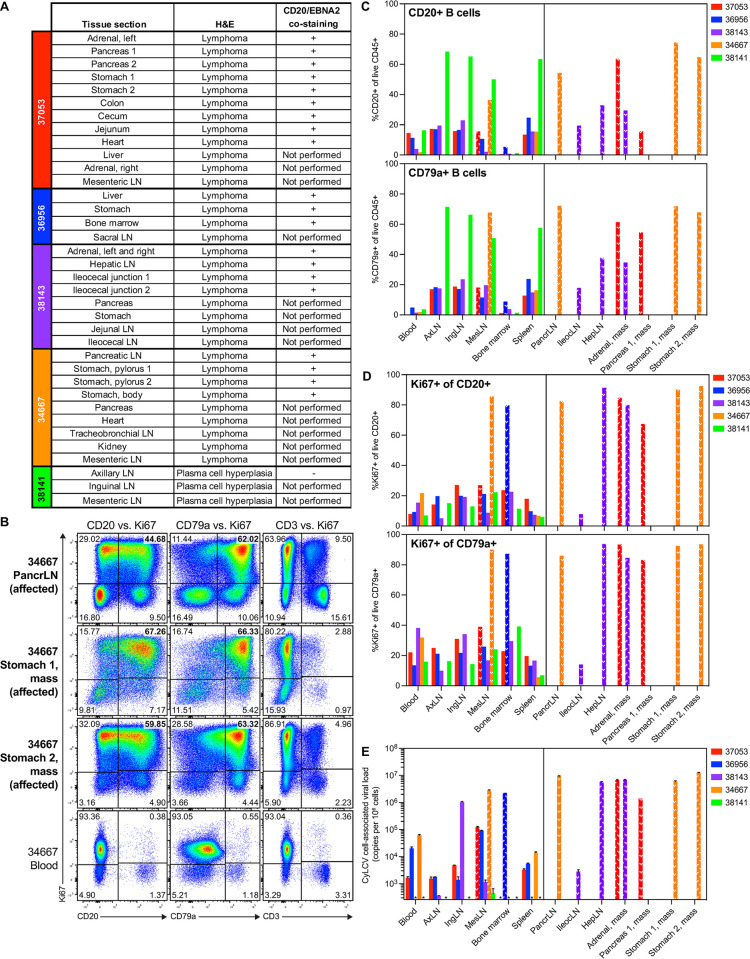
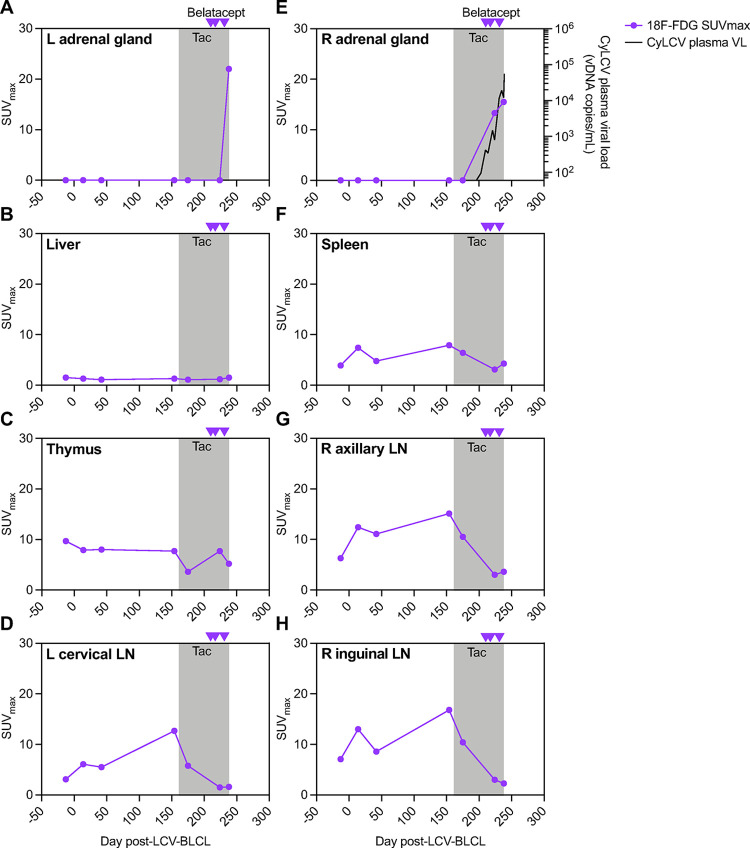
Immunocompromised individuals are at risk for developing lymphocryptovirus-associated lymphoproliferative diseases, such as Epstein Barr virus (EBV)-associated B cell lymphomas and post-transplant lymphoproliferative disorder (PTLD). We previously reported development of cynomolgus lymphocryptovirus (CyLCV)-associated PTLD in Mauritian cynomolgus macaques (MCMs) undergoing hematopoietic stem cell transplantation (HSCT), which mirrored EBV-PTLD in transplant patients. Here, we sought to develop a MCM model of lymphocryptovirus-associated lymphoproliferative disease in immunosuppressed MCMs without HSCT. Five simian immunodeficiency virus (SIV)-infected, CD8α+ cell-depleted MCMs received an infusion of autologous B-lymphoblastoid cells transformed with CyLCV, followed by varying degrees of immunosuppression. Four of five infused macaques developed masses coincident with increasing CyLCV plasma viremia, and necropsies confirmed the presence of multicentric lymphomas, which most commonly manifested in lymph nodes, gastrointestinal tract, adrenal glands, and pancreas. Affected tissues harbored neoplastic lymphocytes double-positive for CD20 and CyLCV EBNA2 antigen, large frequencies of proliferating B cells, and high levels of cell-associated CyLCV DNA. In addition, longitudinal 18F-fluorodeoxyglucose positron-emission tomography (18F-FDG PET) of one MCM successfully detected lymphoproliferative disease in the adrenal glands prior to clinical signs of disease. These data demonstrate successful induction of lymphocryptovirus-associated PTLD-like disease in 4 of 5 MCMs, and thus support the use of MCMs as a preclinical NHP model of EBV-associated lymphoproliferative disease that could be employed to test novel diagnostic and therapeutic modalities.
Copyright: © 2024 Wu et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
