

Systematic review of risk prediction tools for primary cutaneous melanoma outcomes and validation of sentinel lymph node positivity prediction in a UK tertiary cohort
- PMID: 39528626
- PMCID: PMC11554800
- DOI: 10.1038/s44276-024-00110-5
Systematic review of risk prediction tools for primary cutaneous melanoma outcomes and validation of sentinel lymph node positivity prediction in a UK tertiary cohort
Abstract
Background: It is difficult for clinicians to make predictions for cancer progression or outcomes based on AJCC staging for individual patients. Models individualising risk prediction for clinical outcomes are developed using patient level data, advanced statistical techniques, and artificial intelligence.
Methods: A systematic search identified cutaneous melanoma prognostic prediction tools published between January 1985-March 2023. Population comparisons of key clinico-pathological variables, external prediction of receiver operating characteristics and calibration analysis are applied to an unselected group of patients undergoing sentinel lymph node biopsy in a UK University hospital setting (n = 1564).
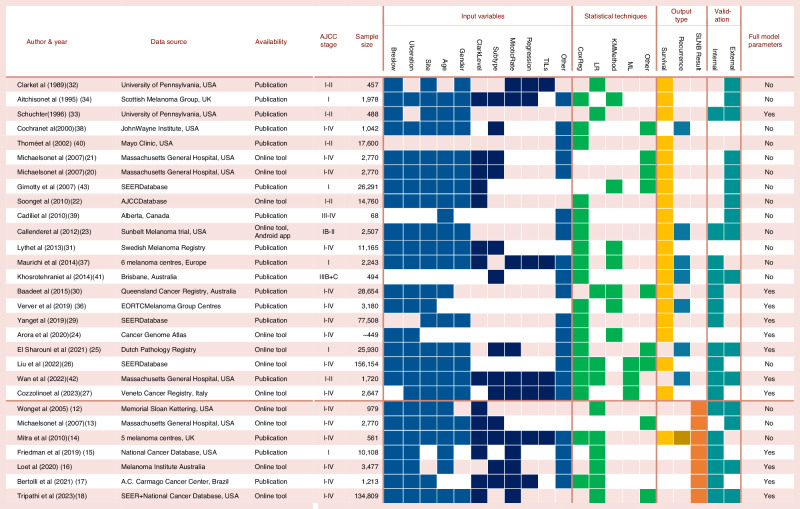
Results: Twenty-nine models were identified which predicted survival, disease recurrence or sentinel lymph node positivity (Internal validation n = 19 and external validation n = 14). 3 out of 7 tools for sentinel node positivity were contemporaneous with available characteristics for external validation. External validation of models by Lo et al. Friedman et al. & Bertolli et al. highlighted good discriminative performance (AUC 68.1% (64.5-71.8%), 77.1% (66.8-85.7%) & 68.6% (63.3-74.1%) respectively) but were sub-optimally calibrated for the UK patient cohort (Calibration intercept & slope Friedman: -4.01 & 32.92, Lo: -1.17 & 0.44, Bertolli: -2.75 & 4.88).
Conclusions: This work highlights the complexity of predictive modelling and the rigorous validation process necessary to ensure accurate predictions. Our search highlights a tendency to focus on discriminative performance over calibration, and the possibility for inconsistent predictions when tools are applied to populations with differing characteristics.
© 2024. The Author(s).
Conflict of interest statement
Figures


References
-
- Cancer Research UK. Melanoma skin cancer statistics [Internet]. 2024 [cited 2024 Sep 8]. https://www.cancerresearchuk.org/health-professional/cancer-statistics/s...
-
- Whiteman DC, Baade PD, Olsen CM. More people die from thin melanomas (≤1 mm) than from thick melanomas (>4 mm) in Queensland, Australia. J Investig Dermatol. 2015;135:1190–3. - PubMed
-
- Amin M, Edge S, Greene F, Byrd D, Brookland R, Washington M, et al. editors. AJCC Cancer Staging Manual 8th Edition. 8th ed. Springer; 2017.
-
- Moons KGM, Altman DG, Reitsma JB, Ioannidis JPA, Macaskill P, Steyerberg EW, et al. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): explanation and elaboration. Ann Intern Med. 2015;162:W1–73. - PubMed
-
- PREDICT Breast Cancer [Internet]. [cited 2020 Oct 31]. https://breast.predict.nhs.uk/
LinkOut - more resources
Full Text Sources