

Astrocyte transcriptomic changes along the spatiotemporal progression of Alzheimer's disease
- PMID: 39528672
- PMCID: PMC11614739
- DOI: 10.1038/s41593-024-01791-4
Astrocyte transcriptomic changes along the spatiotemporal progression of Alzheimer's disease
Abstract
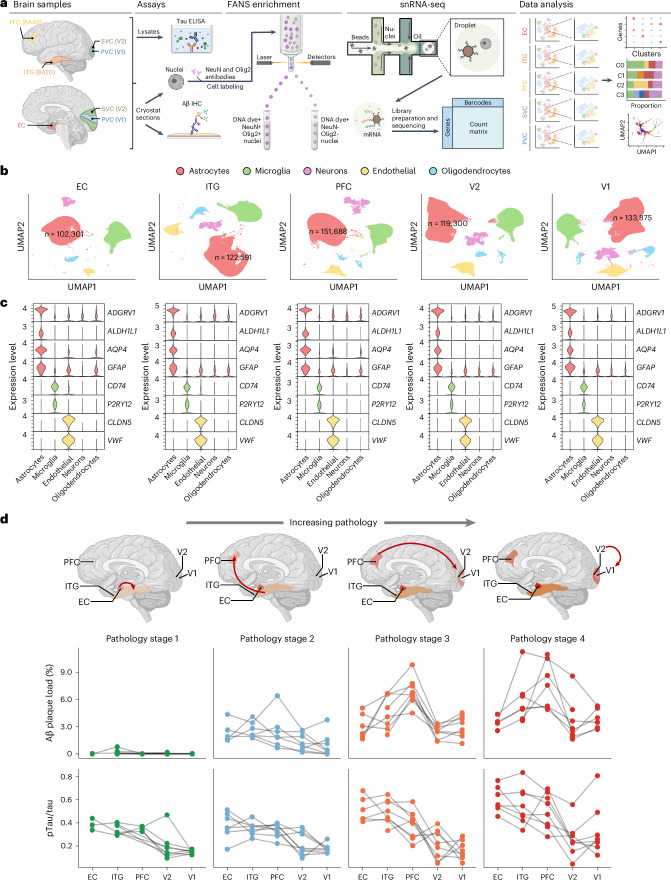
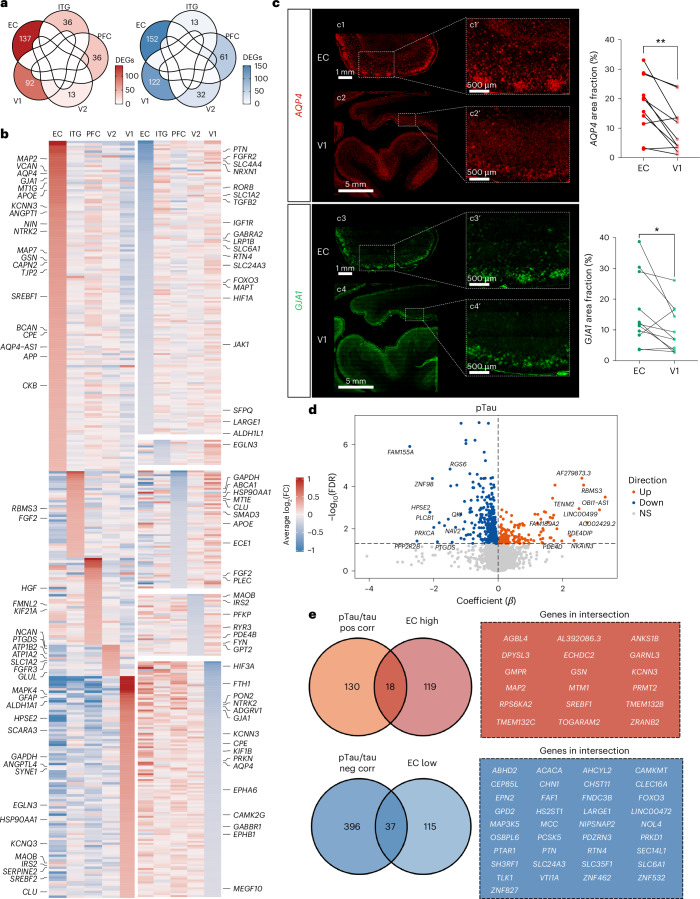
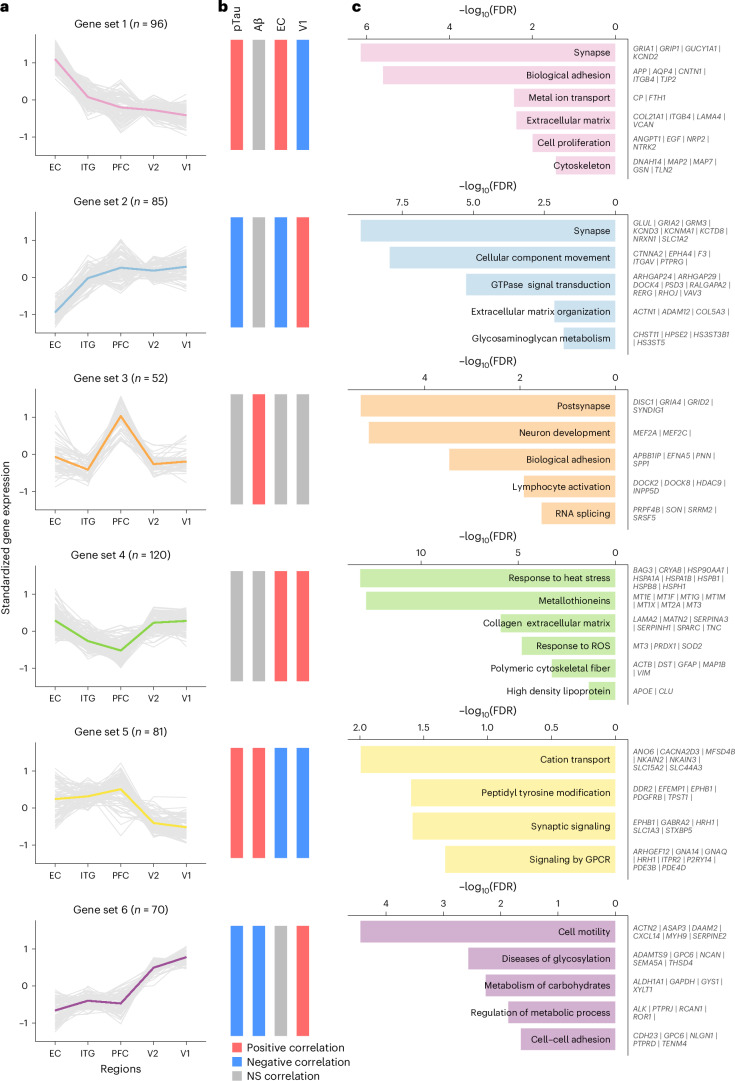
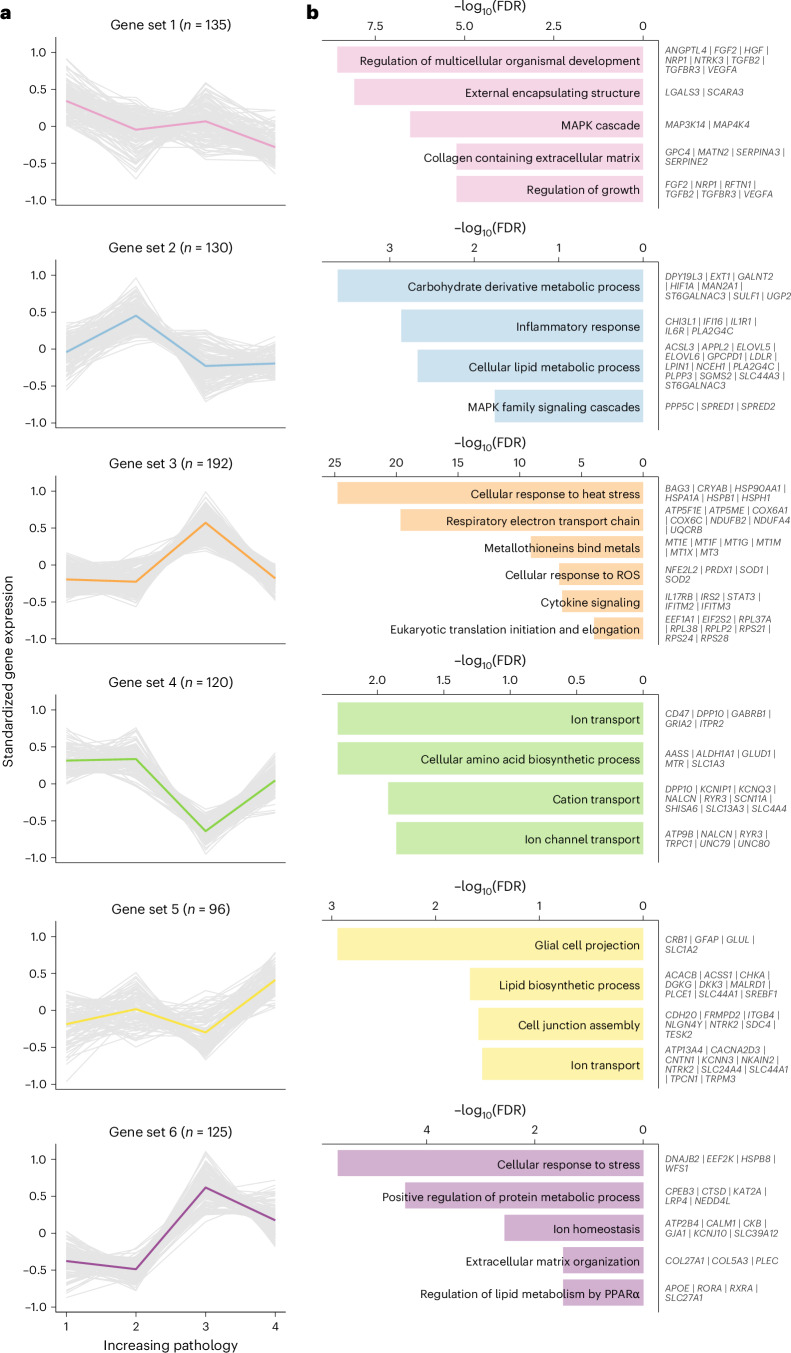
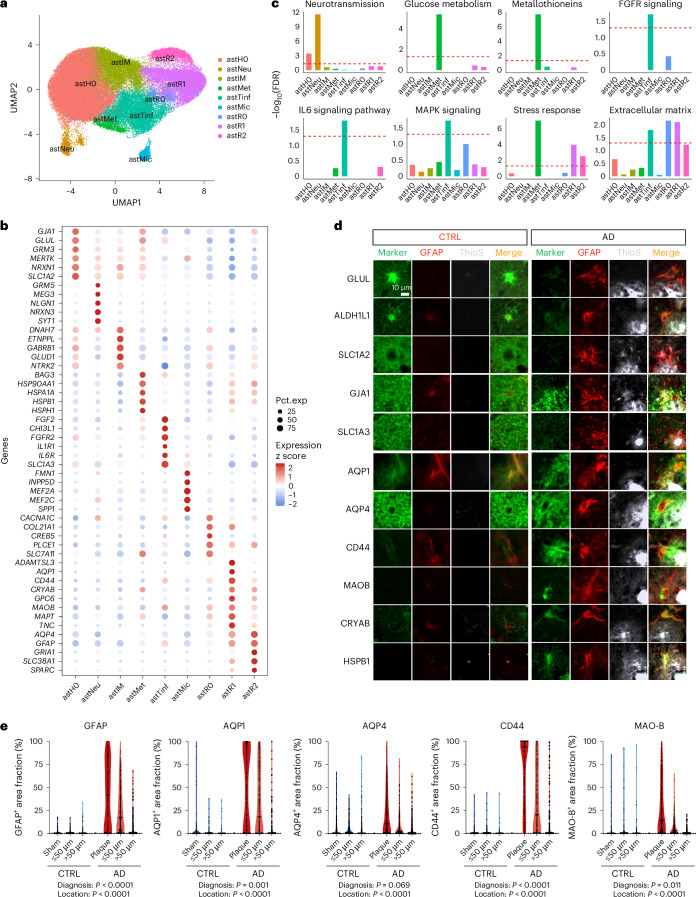
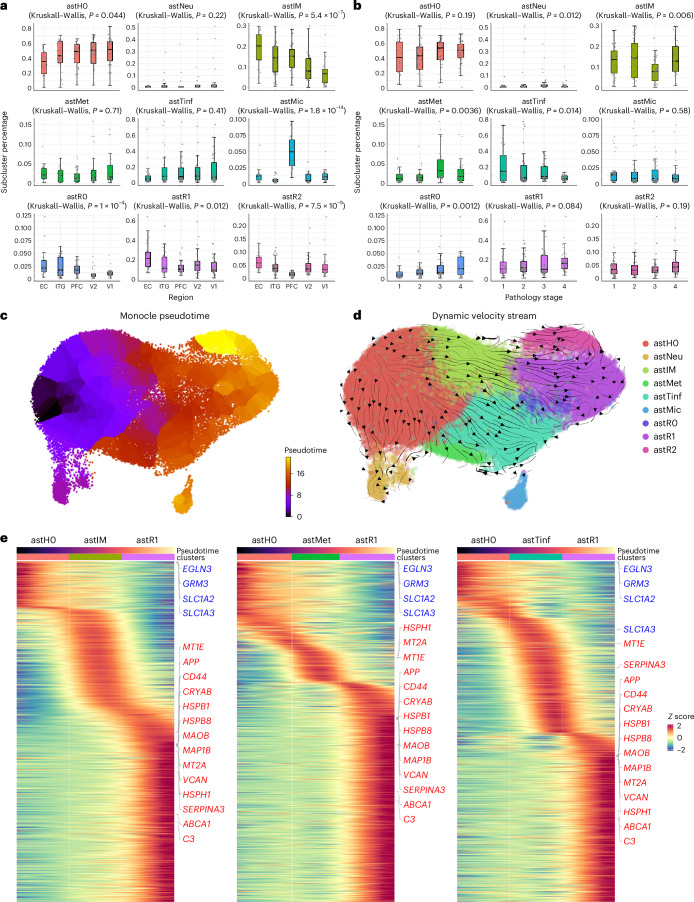
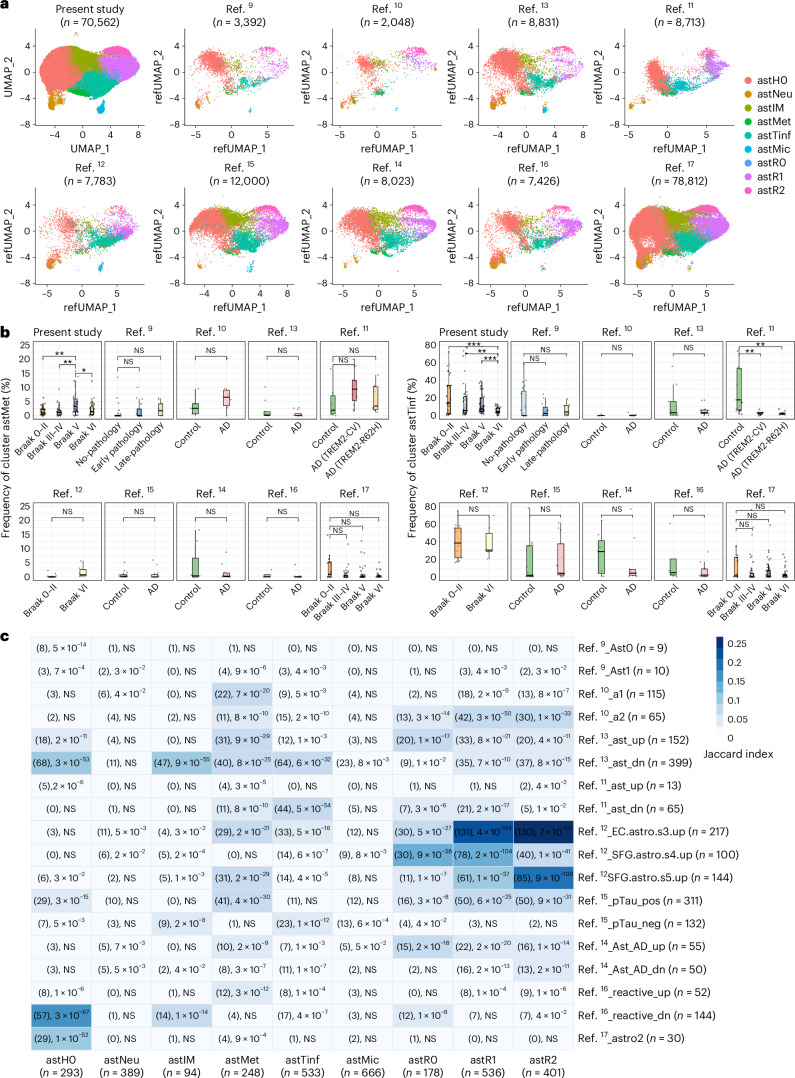
Astrocytes are crucial to brain homeostasis, yet their changes along the spatiotemporal progression of Alzheimer's disease (AD) neuropathology remain unexplored. Here we performed single-nucleus RNA sequencing of 628,943 astrocytes from five brain regions representing the stereotypical progression of AD pathology across 32 donors spanning the entire normal aging to severe AD continuum. We mapped out several unique astrocyte subclusters that exhibited varying responses to neuropathology across the AD-vulnerable neural network (spatial axis) or AD pathology stage (temporal axis). The proportion of homeostatic, intermediate and reactive astrocytes changed only along the spatial axis, whereas two other subclusters changed along the temporal axis. One of these, a trophic factor-rich subcluster, declined along pathology stages, whereas the other increased in the late stage but returned to baseline levels in the end stage, suggesting an exhausted response with chronic exposure to neuropathology. Our study underscores the complex dynamics of astrocytic responses in AD.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: M.E.W., A.W., K.Z., F.L., G.L., T.P., J.T., A.A., T.K., R.V.T, K.B. and E.H.K. are employees of Abbvie. The design, study conduct and financial support for this research were provided by Abbvie. Abbvie participated in the interpretation of data, review and approval of the publication. B.T.H. has a family member who works at Novartis and owns stock in Novartis, serves on the scientific advisory board of Dewpoint and owns stock, serves on a scientific advisory board or is a consultant for Abbvie, Arvinas, Biogen, Novartis, Cell Signaling Technologies, Sangamo, Sanofi, Takeda, US Department of Justice and Vigil, and his laboratory is supported by sponsored research agreements with Abbvie, F Prime and Spark. The remaining authors declare no competing interests.
Figures
References
-
- Orre, M. et al. Isolation of glia from Alzheimer’s mice reveals inflammation and dysfunction. Neurobiol. Aging35, 2746–2760 (2014). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
