

Application of mathematical models on efficiency evaluation and intervention of medical institutions in China
- PMID: 39529103
- PMCID: PMC11552179
- DOI: 10.1186/s12913-024-11729-y
Application of mathematical models on efficiency evaluation and intervention of medical institutions in China
Abstract
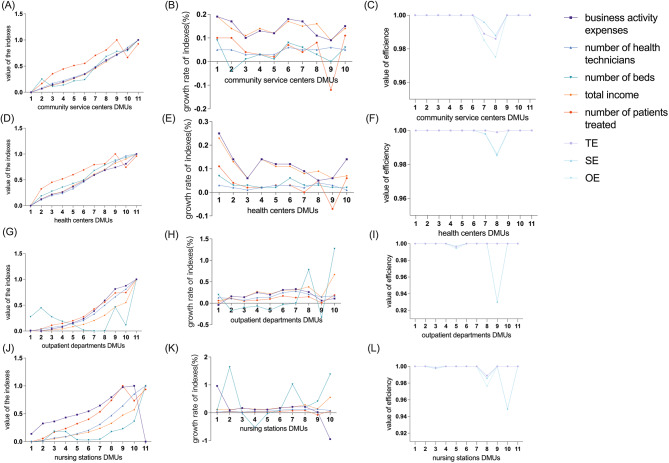
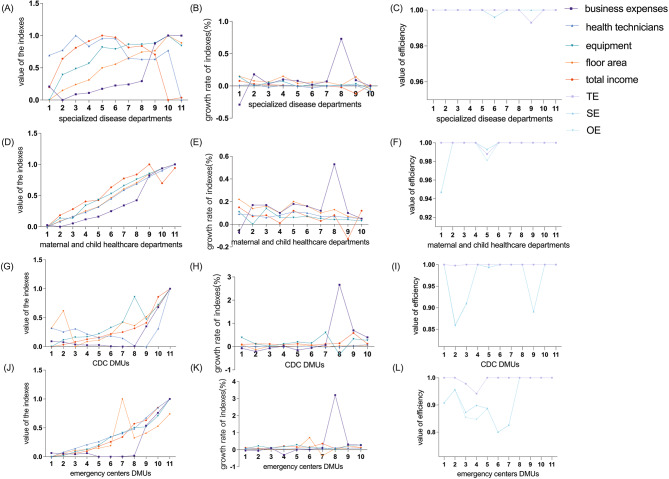
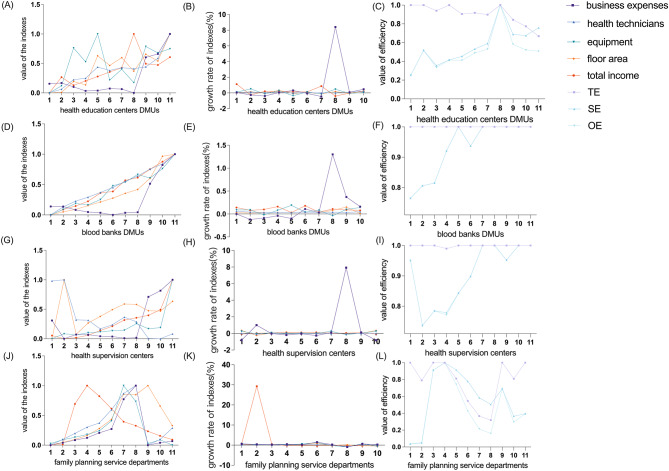
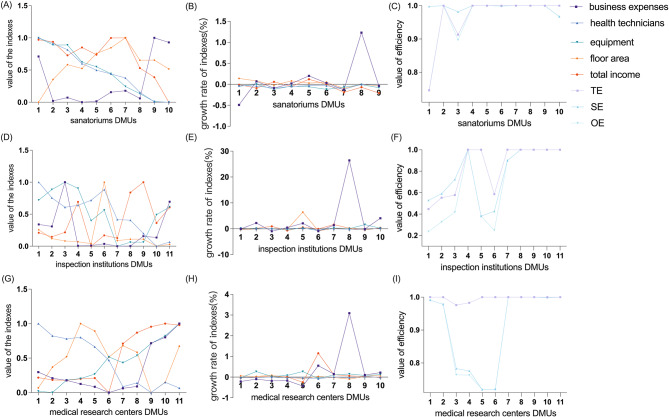
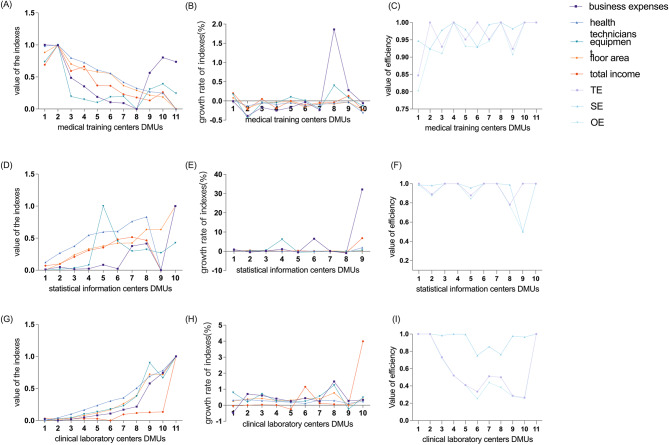
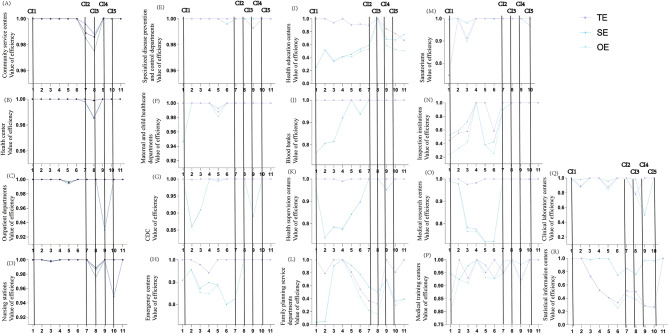
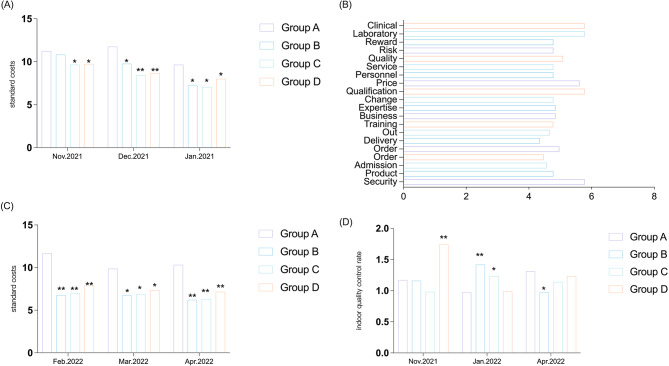
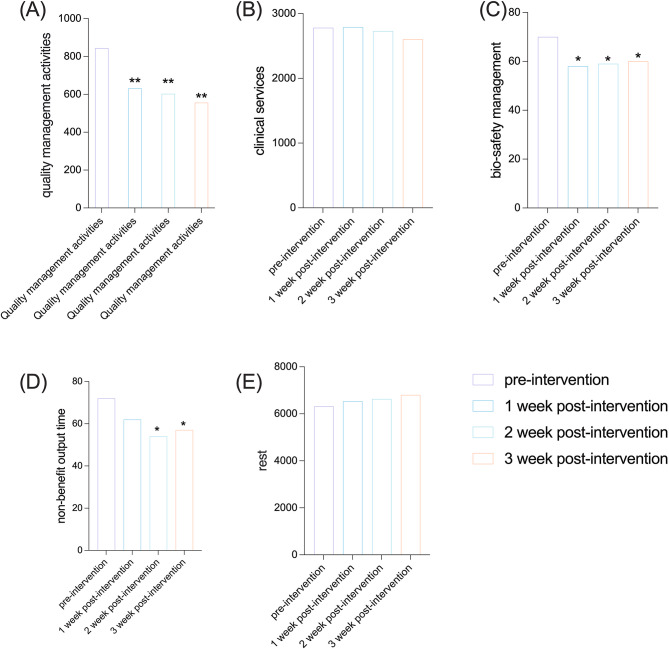
BACKGROUND : The efficiency of medical services directly impacts the economic burden of healthcare, making it crucial to analyze the input-output efficiency of various types of medical institutions. However, while hospitals had been extensively analyzed for their efficiency, other types of medical institutions had received limited attention in this regard. METHODS : In this study, we employed data envelopment analysis (DEA) methods based on time series and internal benchmarks to autonomously assess the efficiency of 18 distinct categories of healthcare facilities in China over the past decade. The verification was conducted through the utilization of the critical incident technique (CIT). Additionally, we utilized the Delphi process (AHP) method to evaluate suppliers of medical consumables, implemented a multi-population genetic algorithm for managing these consumethod and analytic hierarchymables efficiently, and applied stakeholder theory to manage medical personnel efficiency. RESULTS : Our findings indicated that medical institutions capable of providing clinical services exhibited higher levels of efficiency compared to those unable to do so. Multiple indicators suggested redundancy within these institutions. Notably, comprehensive benefit evaluation revealed that clinical laboratory had performed poorly over the past decade. We selected an inefficient medical institution for intervention in reagent management and the work efficiency of medical staff. After implementing the Delphi method and multi-population genetic algorithm for consumable replenishment, the reagent cost was reduced by 40%, 39% and 31% respectively in each of the three experimental groups, compared to the control group. By applying stakeholder theory and process reengineering methods, we were able to shorten quality control management time for medical staff in the experimental group by 41 min per day, reduce clinical service time by 25 min per day, and extend rest time by 70 min per day, while the quality indicators were all meeting the targets. CONCLUSION: By employing various mathematical models as described above, we were able to reduce costs associated with medical consumables and enhance medical personnel work efficiency without compromising quality objectives.
Keywords: AHP; CIT; DEA; Delphi; Medical consumable; Medical institution; Medical personnel efficiency; Multi-population genetic algorithm; Stakeholder.
© 2024. The Author(s).
Conflict of interest statement
Figures
Similar articles
-
Evaluation of healthcare efficiency in China: a three-stage data envelopment analysis of directional slacks-based measure.Front Public Health. 2024 May 30;12:1393143. doi: 10.3389/fpubh.2024.1393143. eCollection 2024. Front Public Health. 2024. PMID: 38873304 Free PMC article.
-
Study on Equity and Efficiency of Health Resources and Services Based on Key Indicators in China.PLoS One. 2015 Dec 17;10(12):e0144809. doi: 10.1371/journal.pone.0144809. eCollection 2015. PLoS One. 2015. PMID: 26679187 Free PMC article.
-
Measuring and Benchmarking Technical Efficiency of Public Hospitals in Tianjin, China: A Bootstrap-Data Envelopment Analysis Approach.Inquiry. 2015 Sep 21;52:0046958015605487. doi: 10.1177/0046958015605487. Print 2015. Inquiry. 2015. PMID: 26396090 Free PMC article.
-
How to evaluate surgical tourism service organizations in China: indicators system development and a pilot application.Glob Health Res Policy. 2022 Aug 16;7(1):26. doi: 10.1186/s41256-022-00262-2. Glob Health Res Policy. 2022. PMID: 35971140 Free PMC article. Review.
-
The Application of Data Envelopment Analysis to Emergency Departments and Management of Emergency Conditions: A Narrative Review.Healthcare (Basel). 2023 Sep 14;11(18):2541. doi: 10.3390/healthcare11182541. Healthcare (Basel). 2023. PMID: 37761738 Free PMC article. Review.
Cited by
-
Association Between Hospital Efficiency and Quality of Care Among Fee-for-Service Medicare Beneficiaries with Prostate Cancer: A Retrospective Cohort Study.Cancers (Basel). 2024 Dec 13;16(24):4154. doi: 10.3390/cancers16244154. Cancers (Basel). 2024. PMID: 39766054 Free PMC article.
References
-
- Chen Z, Shi J, Xu M, Mao L. Efficiency evaluation of surgical nursing wards based on data envelopment analysis. J Nurs Manag. 2022;30(7):3218–26. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
