

Multicentre analysis of seizure outcome predicted by removal of high-frequency oscillations
- PMID: 39530262
- PMCID: PMC12073983
- DOI: 10.1093/brain/awae361
Multicentre analysis of seizure outcome predicted by removal of high-frequency oscillations
Abstract
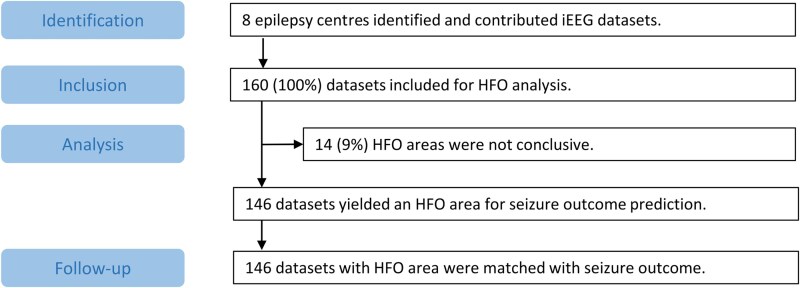
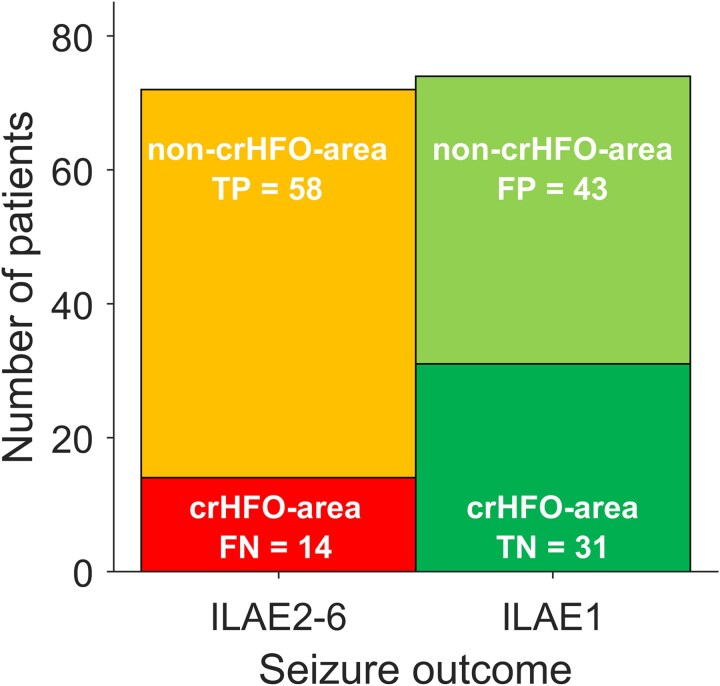
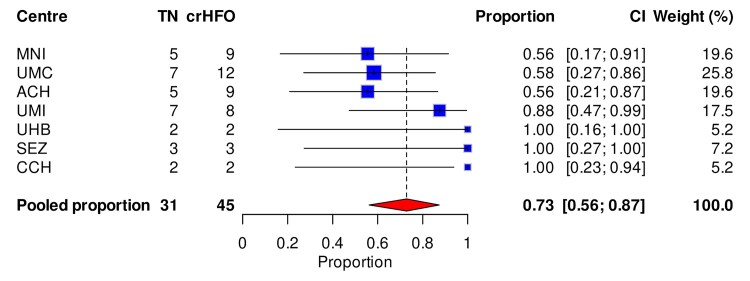
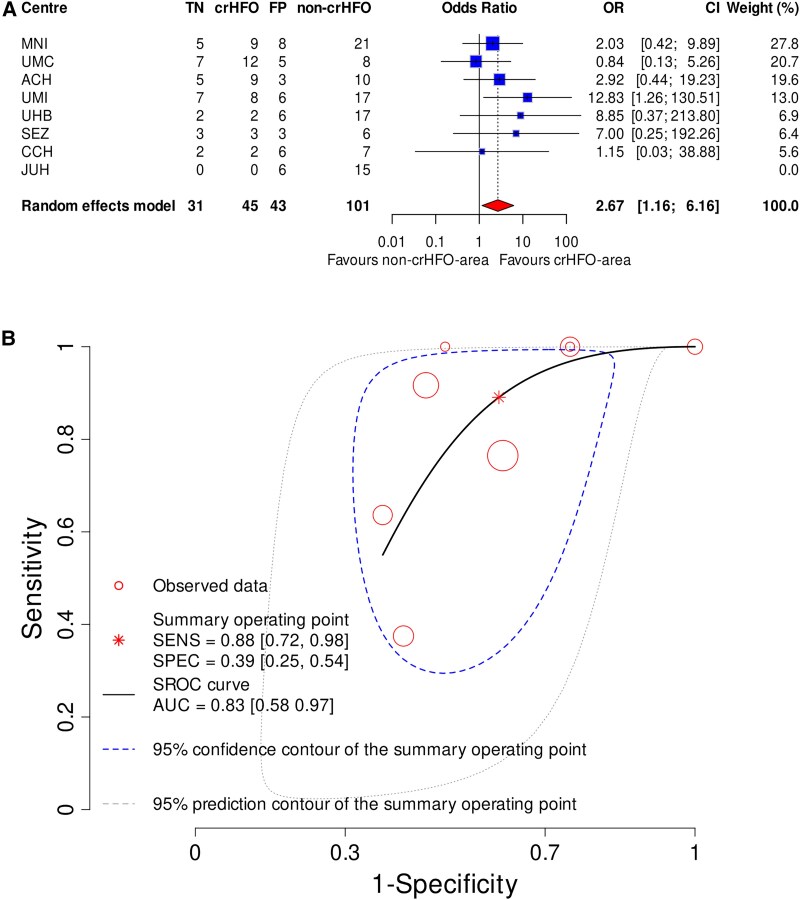
In drug-resistant focal epilepsy, planning surgical resection can involve presurgical intracranial EEG (iEEG) recordings to detect seizures and other iEEG patterns to improve postsurgical seizure outcome. We hypothesized that resection of tissue generating interictal high-frequency oscillations (HFOs, 80-500 Hz) in the iEEG predicts surgical outcome. In eight international epilepsy centres, iEEG was recorded during the presurgical evaluation of patients. The patients were of all ages, had epilepsy of all types, and underwent surgical resection of a single focus aiming at seizure freedom. In a prospective analysis, we applied a fully automated definition of HFO that was independent of the dataset. Using an observational cohort design that was blinded to postsurgical seizure outcome, we analysed HFO rates during non-rapid-eye-movement sleep. If channels had consistently high rates over multiple epochs, they were labelled the 'HFO area'. After HFO analysis, centres provided the electrode contacts located in the resected volume and the seizure outcome at follow-up ≥24 months after surgery. The study was registered at www.clinicaltrials.gov (NCT05332990). We received 160 iEEG datasets. In 146 datasets (91%), the HFO area could be defined. The patients with a completely resected HFO area were more likely to achieve seizure freedom in comparison to those without [odds ratio 2.61, 95% confidence interval (CI) 1.15-5.91, P = 0.02]. Among seizure-free patients, the HFO area was completely resected in 31 and not completely resected in 43. Among patients with recurrent seizures, the HFO area was completely resected in 14 and not completely resected in 58. When predicting seizure freedom, the negative predictive value of the HFO area (68%, CI 52-81) was higher than that for the resected volume as a predictor by itself (51%, CI 42-59, P = 4 × 10-5). The sensitivity and specificity for complete HFO area resection were 0.88 (CI 0.72-0.98) and 0.39 (CI 0.25-0.54), respectively, and the area under the curve was 0.83 (CI 0.58-0.97), indicating good predictive performance. In a blinded cohort study from independent epilepsy centres, applying a previously validated algorithm for HFO marking without the need for adjusting to new datasets allowed us to validate the clinical relevance of HFOs to plan the surgical resection.
Keywords: automated detection; epilepsy surgery; fast ripples; intracranial EEG; ripples.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
J.S. is member of the scientific advisory board of inomed Medizintechnik GmbH. W.S. and S.G. have a licensing agreement with Natus Medical, Inc. inomed, Natus, UCB, Eisai and Medtronic had no involvement in this study.
Figures
References
-
- Ryvlin P, Rheims S. Predicting epilepsy surgery outcome. Curr Opin Neurol. 2016;29:182–188. - PubMed
-
- Rosenow F, Luders H. Presurgical evaluation of epilepsy. Brain. 2001;124(Pt 9):1683–1700. - PubMed
-
- Wieser HG, Blume WT, Fish D, et al. . ILAE commission report. Proposal for a new classification of outcome with respect to epileptic seizures following epilepsy surgery. Epilepsia. 2001;42:282–286. - PubMed
-
- Frauscher B, Mansilla D, Abdallah C, et al. . Learn how to interpret and use intracranial EEG findings. Epileptic Disord. 2024;26:1–59. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01NS104116/GF/NIH HHS/United States
- PJT-175056/CAPMC/ CIHR/Canada
- R01NS094399/GF/NIH HHS/United States
- K12NS098482/GF/NIH HHS/United States
- R01NS134944/GF/NIH HHS/United States
- K01 ES026839/ES/NIEHS NIH HHS/United States
- R01 NS094399/NS/NINDS NIH HHS/United States
- Alexander S. Onassis Public Benefit Foundation
- R01 NS134944/NS/NINDS NIH HHS/United States
- K01-ES026839/GF/NIH HHS/United States
- NU22-08-00278/Ministry of Health of the Czech Republic
- 803880/ERC
- 2015096/Doris Duke Foundation
- K12 NS098482/NS/NINDS NIH HHS/United States
- 09150172210057/VIDI
- SNSF 204651/SNSF_/Swiss National Science Foundation/Switzerland
- NEF17-07/EpilepsieNL
- Universität Zürich
- R01 NS104116/NS/NINDS NIH HHS/United States
- LSHM19080/Health-Holland
LinkOut - more resources
Full Text Sources
Medical
