

Type 2 diabetes pathway-specific polygenic risk scores elucidate heterogeneity in clinical presentation, disease progression and diabetic complications in 18,217 Chinese individuals with type 2 diabetes
- PMID: 39531041
- PMCID: PMC11832604
- DOI: 10.1007/s00125-024-06309-y
Type 2 diabetes pathway-specific polygenic risk scores elucidate heterogeneity in clinical presentation, disease progression and diabetic complications in 18,217 Chinese individuals with type 2 diabetes
Abstract
Aims/hypothesis: Type 2 diabetes is a complex and heterogeneous disease and the aetiological components underlying the heterogeneity remain unclear in the Chinese and East Asian population. Therefore, we aimed to investigate whether specific pathophysiological pathways drive the clinical heterogeneity in type 2 diabetes.
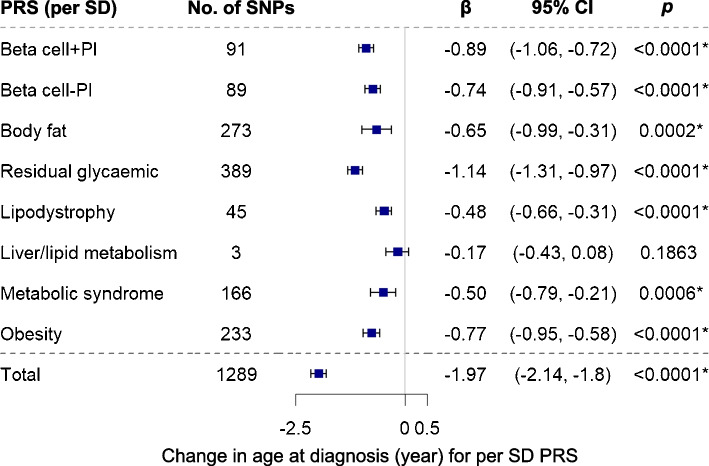
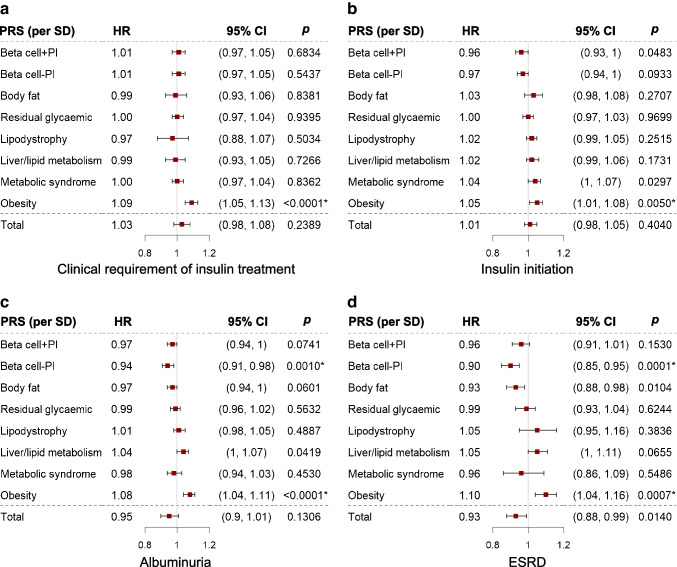
Methods: We employed newly developed type 2 diabetes hard-clustering and soft-clustering pathway-specific polygenic risk scores (psPRSs) to characterise individual genetic susceptibility to pathophysiological pathways implicated in type 2 diabetes in 18,217 Chinese patients from Hong Kong. The 'total' type 2 diabetes polygenic risk score (PRS) was summed by genome-wide significant type 2 diabetes signals (n=1289). We examined the associations between psPRSs and cardiometabolic profile, age of onset, two glycaemic deterioration outcomes (clinical requirement of insulin treatment, defined by two consecutive HbA1c values ≥69 mmol/mol [8.5%] more than 3 months apart during treatment with two or more oral glucose-lowering drugs, and insulin initiation), three renal (albuminuria, end-stage renal disease and chronic kidney disease) outcomes and five cardiovascular outcomes.
Results: Although most psPRSs and total type 2 diabetes PRS were associated with an earlier and younger onset of type 2 diabetes, the psPRSs showed distinct associations with clinical outcomes. In particular, individuals with normal weight showed higher psPRSs for beta cell dysfunction and lipodystrophy than those who were overweight. The psPRSs for obesity were associated with faster progression to clinical requirement of insulin treatment (adjusted HR [95% CI] 1.09 [1.05, 1.13], p<0.0001), end-stage renal disease (1.10 [1.04, 1.16], p=0.0007) and CVD (1.10 [1.05, 1.16], p<0.0001) while the psPRSs for beta cell dysfunction were associated with reduced incident end-stage renal disease (0.90 [0.85, 0.95], p=0.0001) and heart failure (0.83 [0.73, 0.93], p=0.0011). Major findings remained significant after adjusting for a set of clinical variables.
Conclusions/interpretation: Beta cell dysfunction and lipodystrophy could be the driving pathological pathways in type 2 diabetes in individuals with normal weight. Genetic risks of beta cell dysfunction and obesity represent two major genetic drivers of type 2 diabetes heterogeneity in disease progression and diabetic complications, which are shared across ancestry groups. Type 2 diabetes psPRSs may help inform patient stratification according to aetiology and guide precision diabetes care.
Keywords: Chinese population; Diabetic complications; Disease progression; Heterogeneity; Pathway-specific polygenic risk score; Type 2 diabetes.
© 2024. The Author(s).
Conflict of interest statement
Acknowledgements: The authors thank all the participants and investigators of the HKDR and HKDB for their contributions, and the medical and nursing staff of the respective hospitals for their professional input and support. The full lists of team members of the Hong Kong Diabetes Biobank Study Group and the TRANSCEND Consortium are included in the ESM additional information section. Data availability: The list of SNPs used to calculate hard- and soft-clustering psPRSs can be found in ESM Tables 6 and 7. HKDR and HKDB data are not publicly available but may be made available upon reasonable request to the corresponding author. Funding: This work was supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region (CU R4012-18), Research Grants Council Theme-based Research Scheme (T12-402/13N), the University Grants Matching Scheme, a CUHK Direct Grant and the Focused Innovation Scheme. RCWM acknowledges support from a Croucher Foundation Senior Medical Research Fellowship, the Research Committee Postdoctoral Fellowship Scheme, the CUHK Internationalisation Faculty Mobility Scheme and the Provost’s Scheme for PhD scholarship of the Chinese University of Hong Kong. JCNC acknowledges support from the Hong Kong Government Health and Medical Research Fund (CFS-CUHK2), Hong Kong Genome Institute, Chinese University of Hong Kong Research Committee Postdoctoral Fellowship Scheme and Innovation and Technology Commission Research Talent Hub. RAO has a research grant from Randox Ltd on autoimmune disease genetic risk score diagnostics and the University of Exeter licenses know-how to Randox and receives royalties for a type 1 diabetes GRS biochip. Authors’ relationships and activities: JCNC received consultancy fees from Astra Zeneca, Bayer, Boehringer Ingelheim, Celltrion, MSD, Pfizer, Servier and Viatris Pharmaceutical; speaker fees from Astra Zeneca, Bayer, Boehringer Ingelheim, MSD, Merck, Sanofi and Servier; and research grants through her institutions from Applied Therapeutics, Astra Zeneca, Hua Medicine, Lee Powder, Lilly, Merck and Servier. APSK received research grants from Abbott, AstraZeneca, Bayer, Boehringer Ingelheim, Eli-Lilly, Kyowa Kirin and Merck Serono and honoraria for consultancy or giving lectures from Nestle, Novo Nordisk, Pfizer and Sanofi. EYKNC received speaker fees from Sanofi and Novartis and institutional research funding from Sanofi, Medtronic Diabetes and Powder Pharmaceuticals Inc. RCWM has received research funding from Bayer, Boehringer Ingelheim, Novo Nordisk, Roche Diagnostics and Tricida Inc. for carrying out clinical trials or studies; and from AstraZeneca, Bayer, Boehringer Ingelheim, Diachii Sankyo, Kyowa Kirin and Merck for speaker honoraria or consultancy in advisory boards. All proceeds have been donated to the Chinese University of Hong Kong to support diabetes research. JCNC, CKPL, RCWM and W-yS are co-founders of GemVCare, a biotech start-up supported by the Technology Start-up Support Scheme for Universities of the Hong Kong Government Innovation and Technology Commission. RCWM is an advisory board member of the editorial board of Diabetologia. RAO has performed consulting for Janssen, Provention Bio and Sanofi. The authors declare that there are no other relationships or activities that might bias, or be perceived to bias, their work. Contribution statement: GY, CHTT, CKPL, MNW, RAO and RCWM conceptualised and designed the study. CHTT, CKPL, ESHL, RO, H-mL, ACWN, YH, BF, CH, HW, AY, HMC, KFL, SCS, GH, CCT, KPL, JYYL, EYNC, MWT, GK, ITL, JKYL, VTFY, EL, SL, SF, YLC, CCS, EC, APSK, WHT, AOYL, W-yS, JCNC and RCWM contributed to data acquisition. GY, CHTT, ESHL conducted statistical analysis. GY, CHTT, CKPL, MS, ESHL, BF, WHT, MNW, RAO, JCNC and RCWM were involved in data interpretation. GY, RAO and RCWM drafted the manuscript. All authors contributed to the editing, review and critical revision of the manuscript. WHT, W-yS, JCNC, RAO and RCWM contributed to funding acquisition for the study. All authors read and approved the final version to be published. RCWM is the guarantor of this work.
Figures


References
-
- Leslie RD, Ma RCW, Franks PW, Nadeau KJ, Pearson ER, Redondo MJ (2023) Understanding diabetes heterogeneity: key steps towards precision medicine in diabetes. Lancet Diabetes Endocrinol 11(11):848–860. 10.1016/S2213-8587(23)00159-6 - PubMed
MeSH terms
Supplementary concepts
Grants and funding
- Direct Grant/Chinese University of Hong Kong
- Focused Innovation Scheme/Chinese University of Hong Kong
- Internationalisation Faculty Mobility Scheme/Chinese University of Hong Kong
- Provost's Scheme for PhD scholarship of the Chin/Chinese University of Hong Kong
- Research Committee Postdoctoral Fellowship Scheme/Chinese University of Hong Kong
- Research Impact Fund (CU R4012-18)/Research Grants Council, University Grants Committee
- Theme-based Research Scheme (T12-402/13N)/Research Grants Council, University Grants Committee
- University Grants Matching Scheme/Research Grants Council, University Grants Committee
- Health/Food and Health Bureau
- Medical Research Fund (CFS-CUHK2)/Food and Health Bureau
- Croucher Foundation Senior Medical Research Fellow/Croucher Foundation
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
