

Maintenance immunosuppressive therapy in liver transplantation: results from CESIT study, an Italian retrospective cohort study
- PMID: 39532354
- PMCID: PMC11574479
- DOI: 10.1136/bmjopen-2024-087373
Maintenance immunosuppressive therapy in liver transplantation: results from CESIT study, an Italian retrospective cohort study
Abstract
Objectives: To investigate the use of maintenance immunosuppressive treatments following liver transplantation and to compare their risk-benefit profiles in clinical practice.
Design: Retrospective multicentrer cohort study.
Setting: Four Italian regions (Lombardy, Veneto, Lazio, Sardinia).
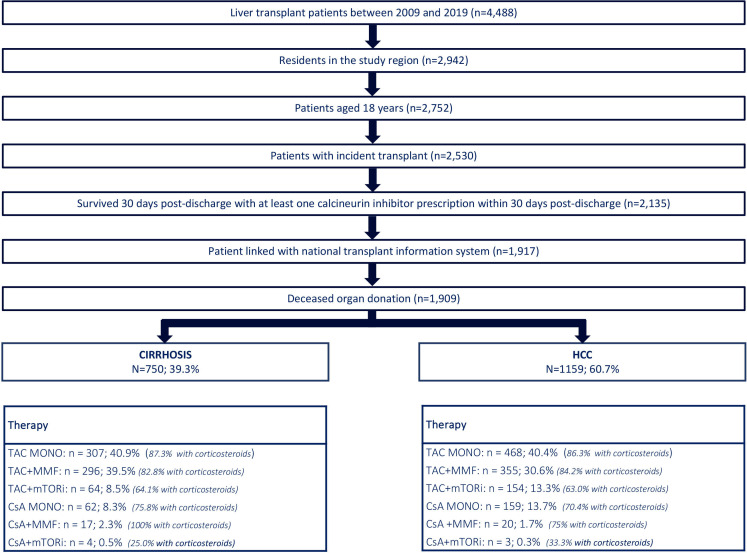
Methods: Data were integrated from the national transplant information system and administrative claims data from four Italian regions. All adults who underwent incident liver transplantation between 2009 and 2019 were identified and categorised into two groups: cirrhosis or hepatocellular carcinoma (HCC). The trend of immunosuppressive treatment over years was analysed, and their effectiveness/safety profiles were compared using multivariate Cox models (HR; 95% CI).
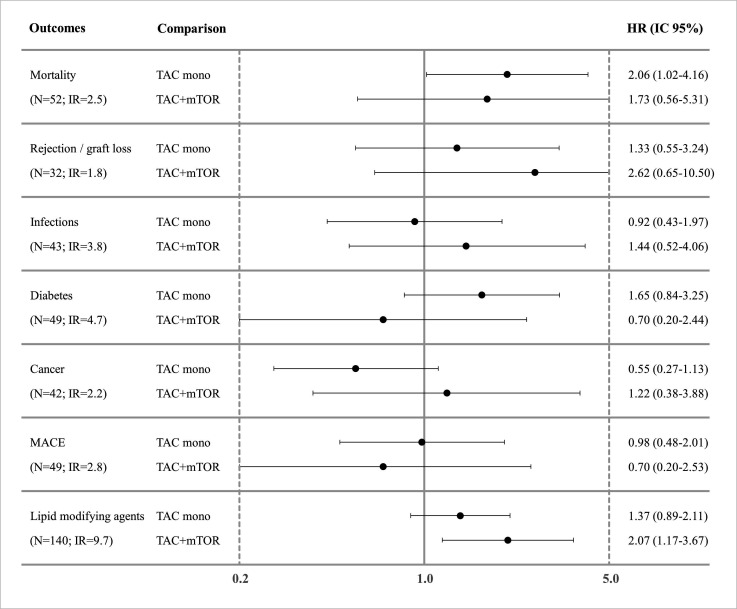
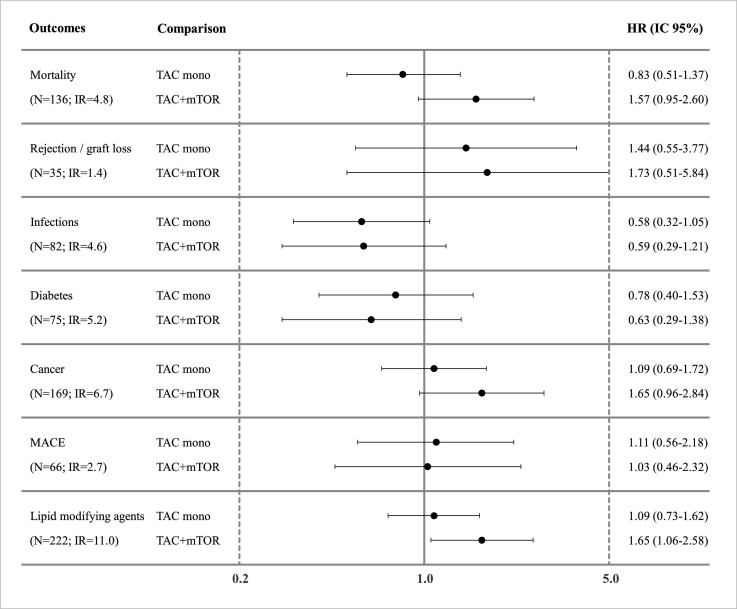
Main outcome measures: Mortality, transplant reject/graft failure, incidence of severe infections, cancer, diabetes, major adverse cardiovascular events and lipid-modifying agents use.
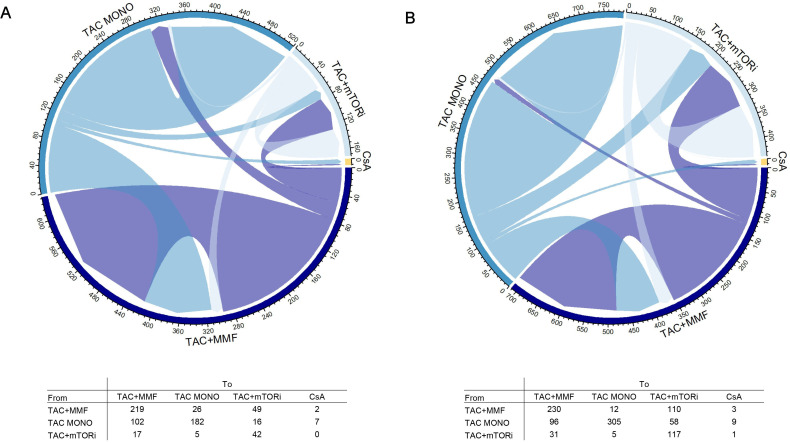
Results: The study comprised 750 subjects in the cirrhosis cohort and 1159 in the HCC cohort. Over the study years, there was a decline in the use of cyclosporine-CsA, while combination therapy involving tacrolimus with other drugs increased compared with monotherapy. Overall, tacrolimus monotherapy use was slightly over 40% in both groups, followed by tacrolimus+mycophenolate (39.5%-cirrhosis; 30.6%-HCC) and tacrolimus+molecular target of rapamycin inhibitors (mTORi) (8.5%-cirrhosis; 13.3%-HCC). No significant differences emerged in risk-benefit profile of different tacrolimus-based therapies, except for a higher risk of mortality in cirrhosis subjects under tacrolimus monotherapy compared with tacrolimus+mycophenolate (HR: 2.07; 1.17 to 3.65).
Conclusions: The study highlights a shift over time in postliver transplant therapeutic patterns, favouring the use of tacrolimus in combination with mycophenolate or mTORi, rather than monotherapy. Moreover, a potential association between tacrolimus monotherapy and increased mortality in the cirrhosis cohort was identified. Further research is warranted to investigate these findings more deeply and to optimise treatment strategies for liver transplant recipients.
Keywords: Drug Therapy; Drug Utilization; EPIDEMIOLOGIC STUDIES; Hepatology; Transplant medicine.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical