

Pain control post total knee replacement in patients given local infiltrative analgesia combined with adductor canal block compared to either modality alone: a systematic review and meta-analysis
- PMID: 39532366
- PMCID: PMC11574392
- DOI: 10.1136/bmjopen-2023-080555
Pain control post total knee replacement in patients given local infiltrative analgesia combined with adductor canal block compared to either modality alone: a systematic review and meta-analysis
Abstract
Objectives: Optimising postoperative pain following knee replacement is important for patients, healthcare professionals and healthcare funders. Adductor canal blocks (ACB) are widely used but there is uncertainty about their efficacy when combined with local infiltration analgesia (LIA) compared with either LIA or ACB alone.
Design: A systematic review and meta-analyses of randomised controlled. The primary outcome was pain over the first 72 hours. Secondary outcomes included morphine use, range of movement, distance walked, length of hospital stay, health economic outcomes and reported adverse events.
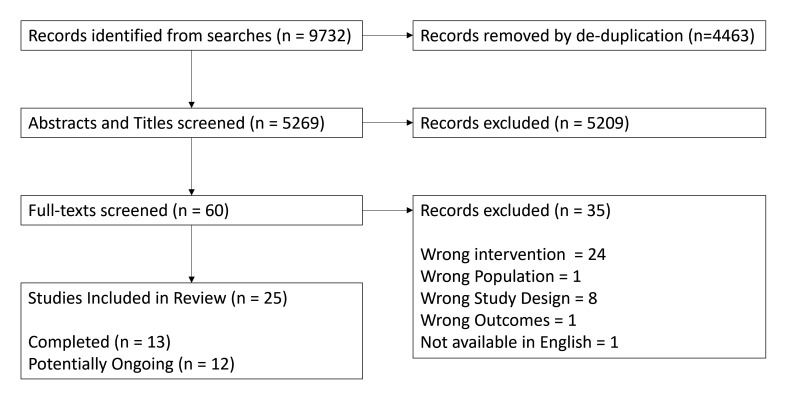
Data sources: MEDLINE, Embase, EB Health - KSR Evidence, Cochrane Central Register of Controlled Trials, CINAHL, International HTA database, ClinicalTrials.gov and the International Clinical Trials Registry Platform (WHO) were searched up to June 2023.
Eligibility criteria: Randomised controlled trials involving patients undergoing primary total knee replacement comparing LIA combined with ACB to either LIA or ACB alone.
Data extraction and synthesis: All eligible studies were data extracted independently by two reviewers. Studies were pooled for each outcome at each timepoint in a random effects meta-analysis.
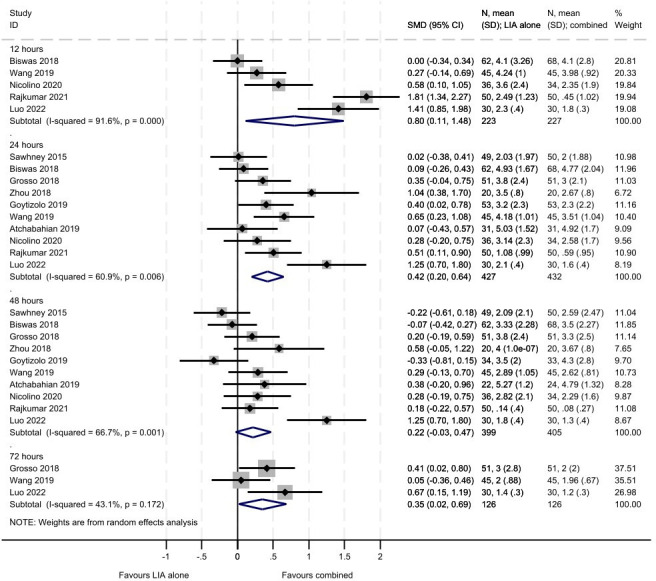
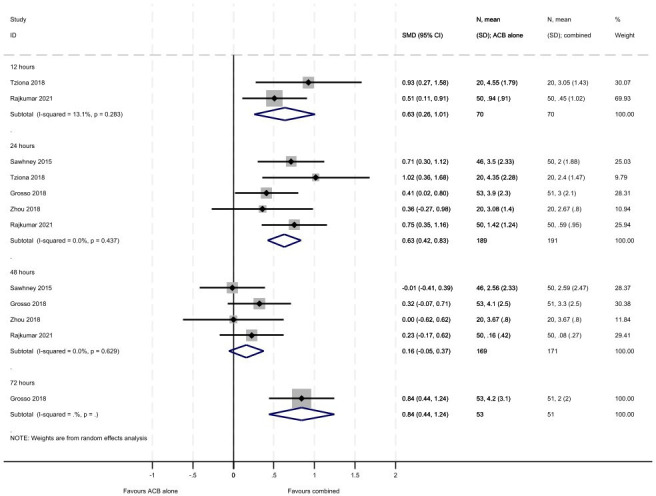
Results: We identified 13 completed studies including 1154 participants. 12 studies compared LIA vs combination and 5 compared ACB vs combination. We identified that participants receiving the combination had lower pain scores at rest at 24 hours compared with LIA alone (SMD 0.42, 95% CI 0.20 to 0.64) or ACB alone (SMD 0.63, 95% CI 0.42 to 0.83). Pain on movement at 24 hours was also lower for patients with combination vs LIA alone (SMD 0.37, 95% CI 0.01 to 0.73) or ACB alone (SMD 0.81, 95% CI 0.35 to 1.26). We also identified that patients on combination used less morphine than on LIA alone (MD 1.06, 95% CI -0.09 to 2.20) or ACB alone (MD 5.94, 95% CI -2.41 to 14.29). The same was seen with range of motion at 24 hours with combination having a larger improvement than LIA alone (MD -5.19, 95% CI -5.55 to -4.83) or ACB alone (MD -3.80, 95% CI -4.37 to -3.23). These findings were consistent across all time points; however, there were no studies deemed to be at a low risk of bias.
Conclusions: Further well-designed and conducted randomised controlled trials are needed to confirm if a combination of LIA and ACB is superior to either option alone for patients undergoing primary total knee arthroplasty.
Prospero registration number: CRD42023436895.
Keywords: Adult surgery; Knee; Meta-Analysis; Pain management; Systematic Review.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: HP has received grants from the NIHR(HTA), NIHR (BRC), Allay Therapeutics, Paradigm Pharma, Depuy Synthes, & Zimmer Biomet. He has received consulting fees from Medacta International, Zimmer Biomet, Invibio, MAT Ortho, Allay Therapeutics, Paradigm Pharma, Microport, & Teleflex. He has also received support to attend meetings from Medacta International, Zimmer Biomet, & Invibio and has received equipment, materials, drugs gifts, or other services from Pacira Pharmaceuticals, Medacta International, & Zimmer Biomet. TH is currently in receipt of a grant from the NIHR.
Figures

References
-
- NJR NJR annual report 2022. The National Joint Registry. 2022. [17-Aug-2023]. https://www.njrcentre.org.uk/njr-annual-report-2022/ Available. Accessed.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical