

Increased Risk of Hypoglycemia Following Roux-en-Y Gastric Bypass Surgery in Patients Without Diabetes: a Propensity Score-Matched Analysis
- PMID: 39532813
- PMCID: PMC11671553
- DOI: 10.1007/s11695-024-07565-y
Increased Risk of Hypoglycemia Following Roux-en-Y Gastric Bypass Surgery in Patients Without Diabetes: a Propensity Score-Matched Analysis
Abstract
Background: Roux-en-Y gastric bypass (RYGB) surgery is an effective treatment for obesity. However, the incidence and long-term risk of hypoglycemia after surgery in patients without diabetes remains unclear. This study aimed to investigate the prevalence of hypoglycemia following RYGB surgery in patients with obesity and without diabetes.
Methods: A retrospective cohort study was conducted using the TriNetX database. The study population included 15,085 patients with obesity (BMI ≥ 30 kg/m2) who underwent RYGB surgery and 3,200,074 non-surgical controls, all without a history of diabetes or GLP-1 receptor agonist use. Propensity score matching was performed to balance baseline characteristics. The primary outcome was the incidence of hypoglycemia, defined by ICD-10-CM codes or laboratory values (glucose ≤ 70 mg/dL). Cox regression analysis was employed to calculate hazard ratios (HR) and 95% confidence intervals (CI).
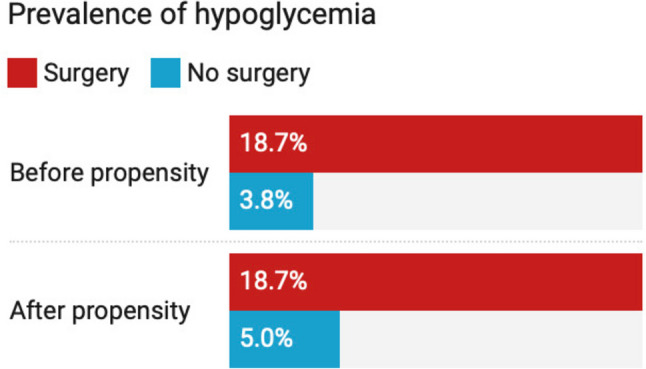
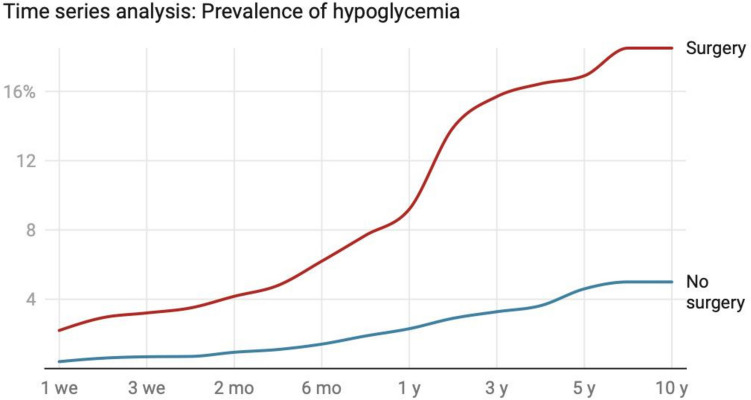
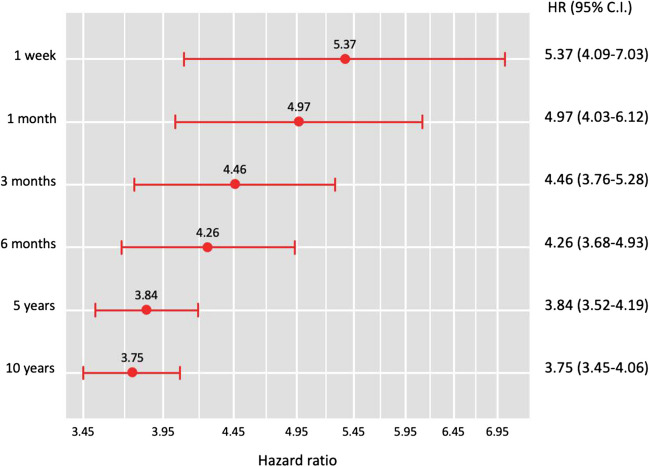
Results: In the overall study population, the risk of hypoglycemia was significantly higher in the RYGB group (18.70%, n = 2,810) compared to the control group (3.80%, n = 120,923; HR 4.3, 95% CI 4.14-4.46, p < 0.001). After propensity score matching (n = 14,916 per group), RYGB patients maintained an elevated risk (18.70%, n = 2,795) compared to matched controls (5.0%, n = 749; HR 3.7, 95% CI 3.44-4.05, p < 0.001). Time-series analysis revealed consistently higher hypoglycemia risk in the RYGB group, with hazard ratios ranging from 5.37 (95% CI 4.09-7.03) at 1 week to 3.75 (95% CI 3.45-4.06) at 10 years post-surgery (all p < 0.001). Subgroup analysis of RYGB patients who developed hypoglycemia showed a 30-day hospitalization rate of 21.3% and a mortality rate of 0.71%.
Conclusion: RYGB surgery is associated with a significantly increased risk of hypoglycemia in patients with obesity and without diabetes, both in the short-term and long-term follow-up. These findings underscore the importance of monitoring and managing hypoglycemia in patients undergoing RYGB surgery, even in the absence of preexisting diabetes.
Keywords: Bariatric surgery; Hypoglycemia; Obesity; Propensity score matching; Roux-en-Y gastric bypass.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Declarations. Competing Interests: The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
