

Seven-year performance of a clinical metagenomic next-generation sequencing test for diagnosis of central nervous system infections
- PMID: 39533109
- PMCID: PMC11645279
- DOI: 10.1038/s41591-024-03275-1
Seven-year performance of a clinical metagenomic next-generation sequencing test for diagnosis of central nervous system infections
Abstract
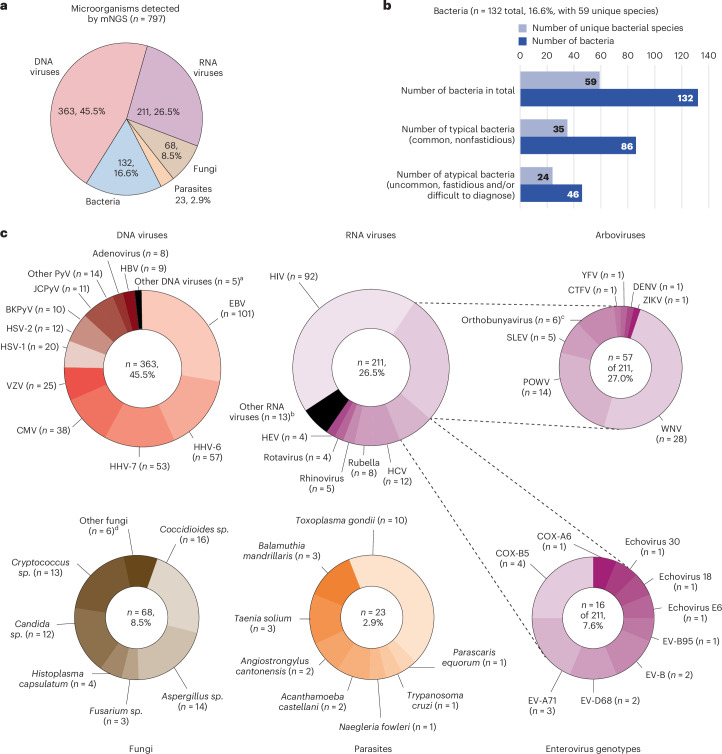
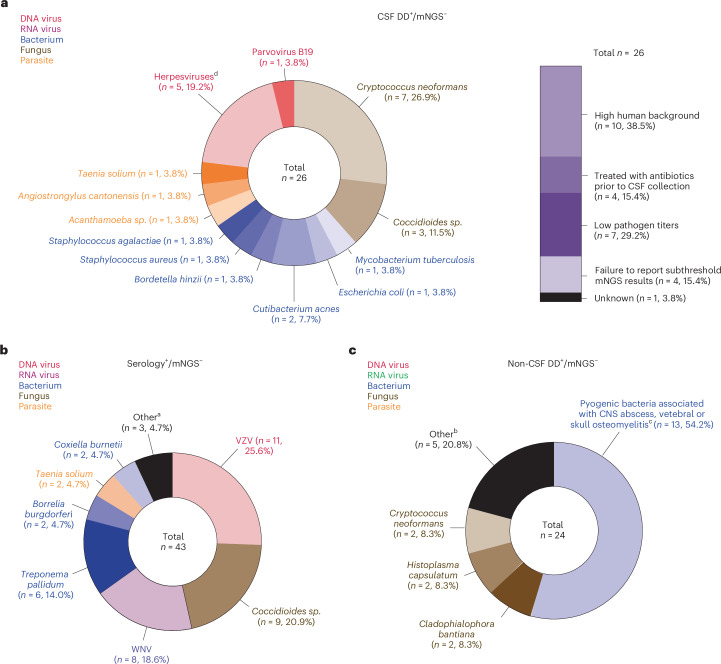
Metagenomic next-generation sequencing (mNGS) of cerebrospinal fluid (CSF) is an agnostic method for broad-based diagnosis of central nervous system (CNS) infections. Here we analyzed the 7-year performance of clinical CSF mNGS testing of 4,828 samples from June 2016 to April 2023 performed by the University of California, San Francisco (UCSF) clinical microbiology laboratory. Overall, mNGS testing detected 797 organisms from 697 (14.4%) of 4,828 samples, consisting of 363 (45.5%) DNA viruses, 211 (26.4%) RNA viruses, 132 (16.6%) bacteria, 68 (8.5%) fungi and 23 (2.9%) parasites. We also extracted clinical and laboratory metadata from a subset of the samples (n = 1,164) from 1,053 UCSF patients. Among the 220 infectious diagnoses in this subset, 48 (21.8%) were identified by mNGS alone. The sensitivity, specificity and accuracy of mNGS testing for CNS infections were 63.1%, 99.6% and 92.9%, respectively. mNGS testing exhibited higher sensitivity (63.1%) than indirect serologic testing (28.8%) and direct detection testing from both CSF (45.9%) and non-CSF (15.0%) samples (P < 0.001 for all three comparisons). When only considering diagnoses made by CSF direct detection testing, the sensitivity of mNGS testing increased to 86%. These results justify the routine use of diagnostic mNGS testing for hospitalized patients with suspected CNS infection.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: A.P.W., B.O., T.B., B.M. and S.M. are employed by and own equity in Delve Bio. C.Y.C. is a co-founder of Delve Bio and on the scientific advisory board for Delve Bio, Flightpath Biosciences, Biomeme, Mammoth Biosciences, BiomeSense and Poppy Health. He is also an inventor on US patent 11380421, ‘Pathogen detection using next-generation sequencing’, under which algorithms for taxonomic classification, filtering and pathogen detection are used by SURPI+ software. C.Y.C. receives research support from Delve Bio and Abbott Laboratories, Inc. M.R.W. is a co-founder and on the scientific advisory board for Delve Bio. The other authors declare no competing interests.
Figures


References
-
- Bloch, K. C., Glaser, C., Gaston, D. & Venkatesan, A. State of the art: acute encephalitis. Clin. Infect. Dis.77, e14–e33 (2023). - PubMed
-
- Zimmer, A. J. et al. Central nervous system infections. Microbiol. Spectr.4, DMIH2-0012-2015 (2016). - PubMed
-
- Koster-Rasmussen, R., Korshin, A. & Meyer, C. N. Antibiotic treatment delay and outcome in acute bacterial meningitis. J. Infect.57, 449–454 (2008). - PubMed
-
- Poissy, J. et al. Factors associated with delay to acyclovir administration in 184 patients with herpes simplex virus encephalitis. Clin. Microbiol. Infect.15, 560–564 (2009). - PubMed
-
- Glaser, C. A. et al. Beyond viruses: clinical profiles and etiologies associated with encephalitis. Clin. Infect. Dis.43, 1565–1577 (2006). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
