

Do patients receiving extracorporeal membrane-oxygenation need antibiotic prophylaxis? A systematic review and meta-analysis on 7,996 patients
- PMID: 39533181
- PMCID: PMC11556216
- DOI: 10.1186/s12871-024-02796-z
Do patients receiving extracorporeal membrane-oxygenation need antibiotic prophylaxis? A systematic review and meta-analysis on 7,996 patients
Abstract
Background: Patients undergoing Extracorporeal Membrane Oxygenation (ECMO) are particularly susceptible to infections: 42% experience sepsis and 26% develop a nosocomial infection (NI). Whether antibiotic prophylaxis is effective in reducing mortality and its effects on the rate of NIs is currently unclear.
Research question: Can antibiotic prophylaxis decrease 30-day mortality for patients on ECMO? Can antibiotic prophylaxis prevent the occurrence of NIs in these patients?
Study design and methods: A systematic review and meta-analysis was conducted. We searched PubMed, Scopus, and CINAHL libraries from inception to June 12, 2024. Two researchers were involved in abstract screening and three researchers were involved in full text selection.
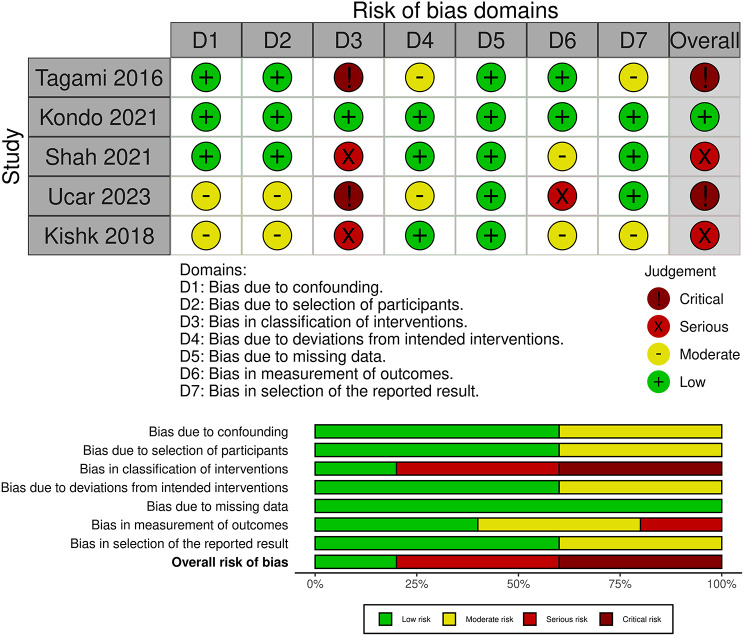
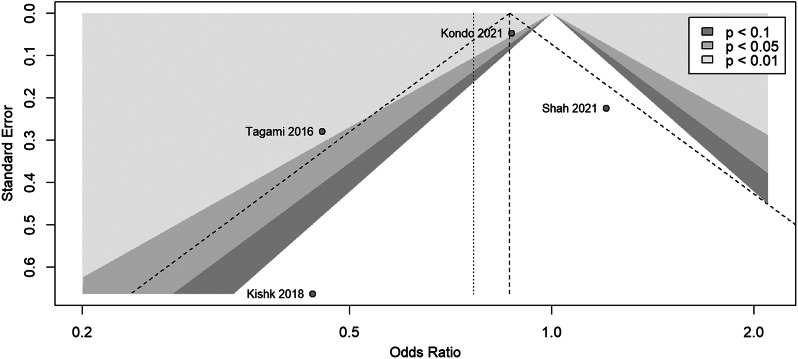
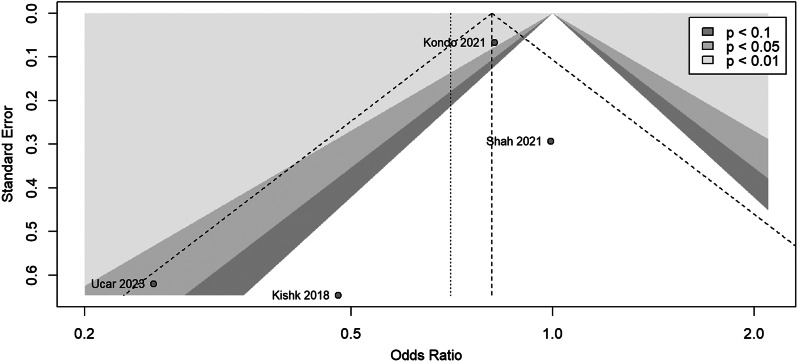
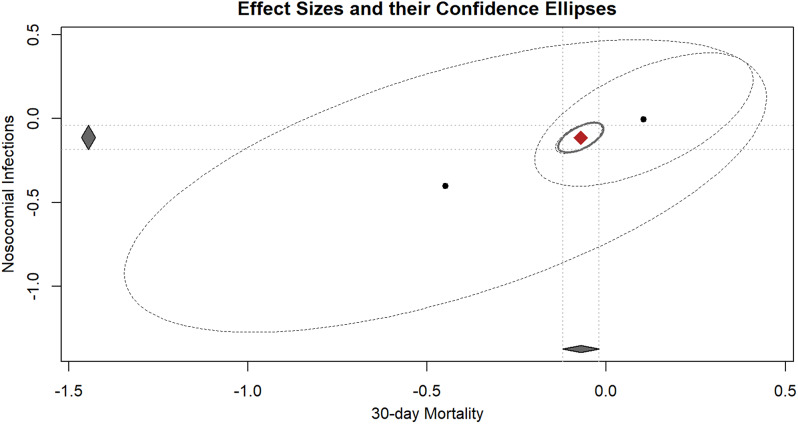
Results: A pooled population of 7,996 patients is represented by 5 retrospective studies. Reported mortality ranges between 46 and 58% and the NIs rate is between 14 and 62%. Regarding 30-day mortality, the random-effects model (I2 = 65%) indicates a non-statistically significant difference between the antibiotic prophylaxis group and the non-prophylaxis group (OR 0.76; 95%CI 0.37-1.59). For the NIs rate, a fixed-effect model (I2 = 36%) shows an OR of 0.81 (95%CI 0.71-0.92) in favor of the antibiotic prophylaxis group, with a number-needed-to-treat (NNT) of 39.7 patients.
Conclusion: According to a very low degree of certainty, antibiotic prophylaxis appears to have no impact on the 30-day mortality rate of ECMO recipients. The risk of NIs seems to decrease with antibiotic prophylaxis, even though the NNT is high. Prospective high-quality studies that address these specific clinical questions are necessary.
Clinical trial registration: PROSPERO: International prospective register of systematic reviews, 2024, CRD42024567037.
Keywords: Antibiotic prophylaxis; ECMO; Meta-analysis; Mortality; Nosocomial infection.
© 2024. The Author(s).
Conflict of interest statement
Figures



Similar articles
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Antibiotic prophylaxis for preventing burn wound infection.Cochrane Database Syst Rev. 2013 Jun 6;2013(6):CD008738. doi: 10.1002/14651858.CD008738.pub2. Cochrane Database Syst Rev. 2013. PMID: 23740764 Free PMC article.
-
Long-term antibiotic prophylaxis for prevention of rheumatic fever recurrence and progression to rheumatic heart disease.Cochrane Database Syst Rev. 2024 Sep 23;9(9):CD015779. doi: 10.1002/14651858.CD015779. Cochrane Database Syst Rev. 2024. PMID: 39312290
-
Antibiotic prophylaxis to prevent spontaneous bacterial peritonitis in people with liver cirrhosis: a network meta-analysis.Cochrane Database Syst Rev. 2020 Jan 16;1(1):CD013125. doi: 10.1002/14651858.CD013125.pub2. Cochrane Database Syst Rev. 2020. PMID: 31978256 Free PMC article.
References
-
- Ait Hssain A, Vahedian-Azimi A, Ibrahim AS, Hassan IF, Azoulay E, Darmon M. Incidence, risk factors and outcomes of nosocomial infection in adult patients supported by extracorporeal membrane oxygenation: a systematic review and meta-analysis. Crit Care. 2024;28(1):158. 10.1186/s13054-024-04946-8. PMID: 38730424; PMCID: PMC11088079. - PMC - PubMed
-
- Bizzarro MJ, Conrad SA, Kaufman DA, Rycus P, Extracorporeal Life Support Organization Task Force on Infections, Extracorporeal Membrane Oxygenation. Infections acquired during extracorporeal membrane oxygenation in neonates, children, and adults. Pediatr Crit Care Med. 2011;12(3):277–81. 10.1097/PCC.0b013e3181e28894. PMID: 20495508. - PubMed
-
- O’Horo JC, Cawcutt KA, De Moraes AG, Sampathkumar P, Schears GJ. The Evidence Base for Prophylactic Antibiotics in Patients Receiving Extracorporeal Membrane Oxygenation. ASAIO J. 2016 Jan-Feb;62(1):6–10. 10.1097/MAT.0000000000000287. PMID: 26461238. - PubMed
-
- ELSO Guidelines | Extracorporeal Membrane Oxygenation (ECMO) (accessed 5th. July 2024).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
