

Are rates of clinical interventions during pregnancy and childbirth different for refugees and asylum seekers in high-income countries? A scoping review
- PMID: 39533211
- PMCID: PMC11558906
- DOI: 10.1186/s12884-024-06893-2
Are rates of clinical interventions during pregnancy and childbirth different for refugees and asylum seekers in high-income countries? A scoping review
Abstract
Background: Adequate maternity care and appropriate clinical interventions during labour and delivery can reduce adverse perinatal outcomes, but unnecessary interventions may cause harm. While studies have shown that refugees and asylum seekers face important barriers when accessing maternity care, there is a lack of high-quality quantitative data on perinatal health interventions, such as induction of labour or caesarean sections, among refugees and asylum seekers and the findings reported in the literature tend to be inconsistent. Our goal was to examine and synthesise the evidence regarding the rates of intrapartum clinical interventions in women who are refugees and asylum seekers in high-income countries compared to other population groups.
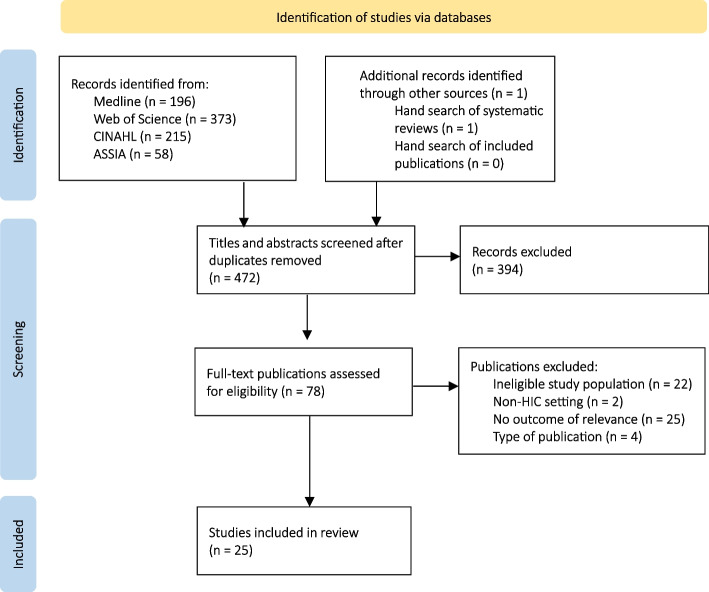
Methods: We conducted a scoping review of peer-reviewed studies published in English since 2011 that report original quantitative findings regarding intrapartum clinical interventions among refugees and asylum seekers in high-income countries compared to those in non refugee, non asylum seeker populations. We examined reported rates of clinical pain relief, labour induction and augmentation, episiotomies, instrumental deliveries, and caesarean sections.
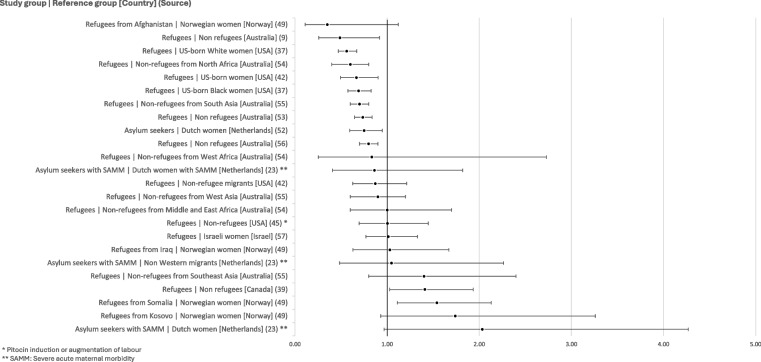
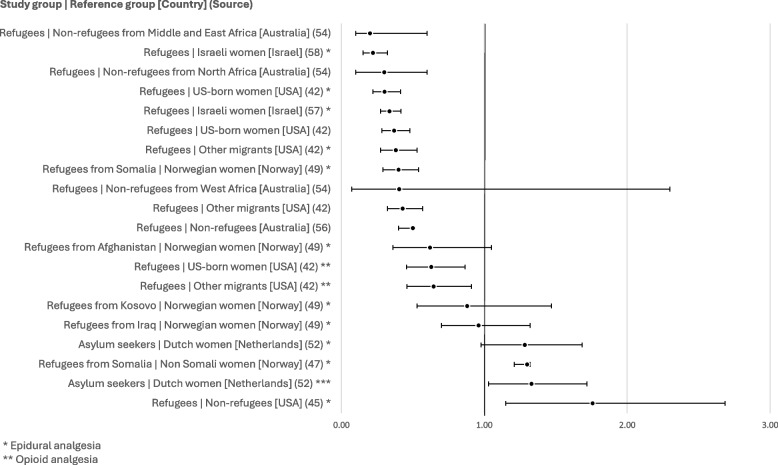
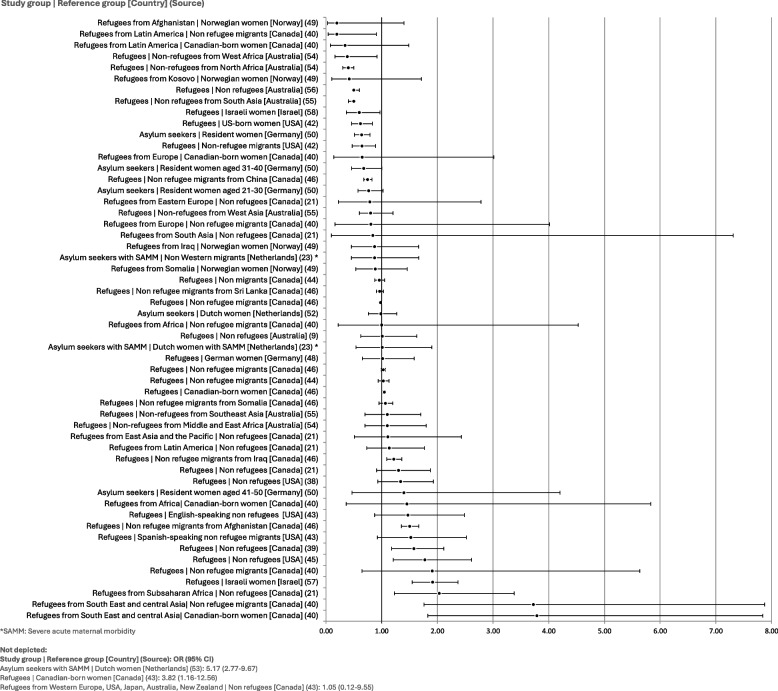
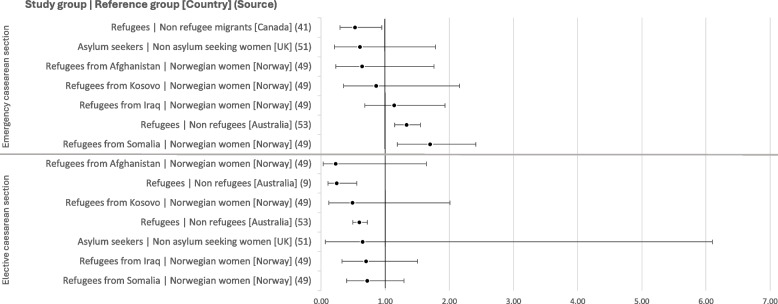
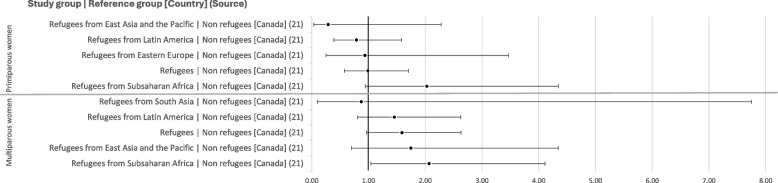
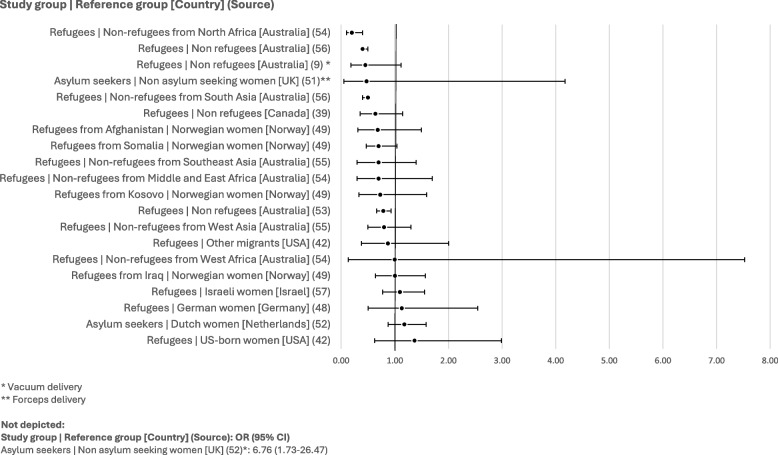
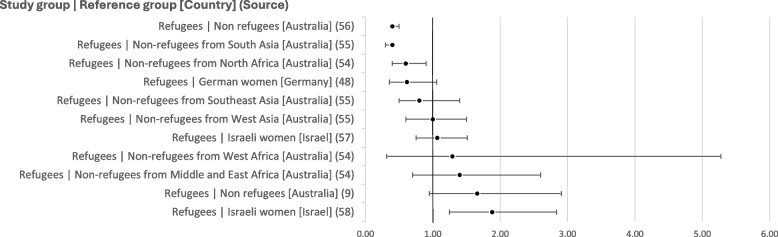
Results: Twenty-five papers were included in the review. Findings indicate that refugees and asylum seekers were less likely to receive pain relief, with 16 out of 20 data points showing unadjusted ORs ranging from 0.20 (CI: 0.10-0.60) to 0.96 (CI: 0.70-1.32). Similarly, findings indicate lower odds of instrumental delivery among refugees and asylum seekers with 14 of 21 data points showing unadjusted ORs between 0.25 (CI: 0.15-0.39) and 0.78 (CI: 0.47-1.30); the remaining papers report no statistically significant difference between groups. There was no discernable trend in rates of labour induction and episiotomies across studies.
Conclusions: The studies included in this review suggest that asylum seekers and refugees are less likely to receive clinical pain relief and experience instrumental delivery than non-refugee groups in high-income countries. This review strengthens our understanding of the links between immigration status and maternity care, ultimately informing policy and practice to improve perinatal health and the provision of care for all.
Keywords: Asylum; Childbirth; Intervention; Intrapartum; Migrant; Refugee.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- United Nations High Commissioner for Refugees. Gobal trends: Forced displacement in 2022. Copenhagen; 2023.
-
- WHO Health and Migration Programme. Promoting the health of refugees and migrants: experiences from around the world. Geneva; 2023.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
