

Evaluation of V-type titanium cable internal fixation for the treatment of young adult fifth lumbar spondylolysis: technical notes and a retrospective clinical study
- PMID: 39533313
- PMCID: PMC11559233
- DOI: 10.1186/s13018-024-05197-7
Evaluation of V-type titanium cable internal fixation for the treatment of young adult fifth lumbar spondylolysis: technical notes and a retrospective clinical study
Abstract
Background: Various strategies, each with its own set of limitations, are available for managing lumbar spondylolysis. In response, our department has developed an innovative solution: a V-shaped titanium cable integrated with a pedicle screw internal fixation system specifically designed for lumbar spondylolysis in young adults.
Aim: The objective of this study was to thoroughly investigate the long-term efficacy of V-type titanium cable internal fixation for the management of spondylolysis, especially in young adults.
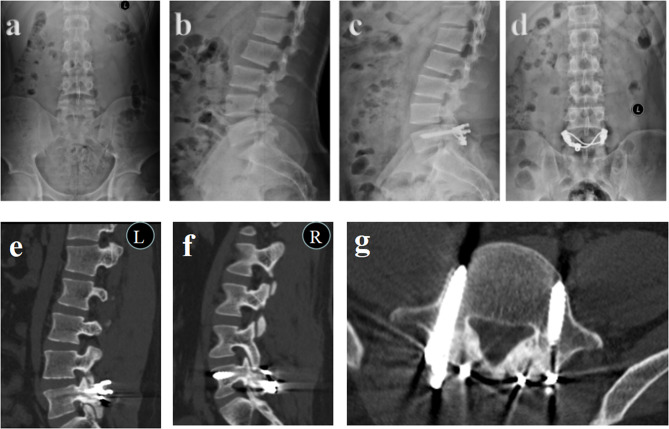
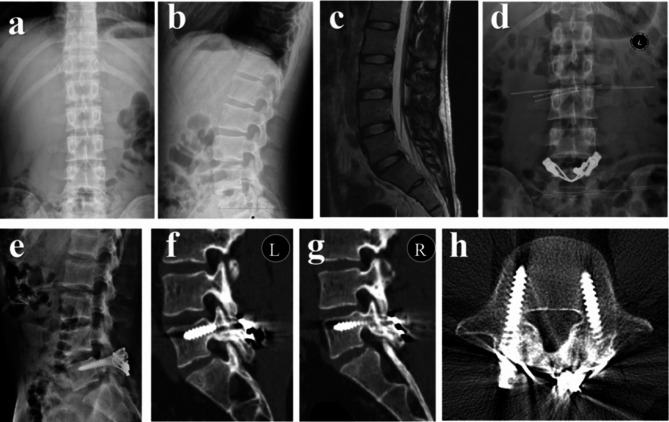
Methods: Twenty-one patients with fifth lumbar spondylolysis were treated using V-shaped titanium cables and pedicle screw internal fixation at the General Hospital Xinjiang Military Command. The duration of low back pain before surgery was 6 ~ 48 (15.85 ± 11.57) months. The Medtronic (S7) navigation system was used during surgery to guide the placement of pedicle screws, aiming to avoid damaging the L4-5 facet joint by positioning the screws lower and further to the side. Intraoperative indices (operative time and intraoperative blood loss) were recorded. The visual analog scale (VAS), Oswestry Disability Index (ODI), pelvic incidence (PI), and intraoperative imaging measurements of screw accuracy were meticulously recorded and assessed in a comprehensive manner. This thorough evaluation was conducted both intraoperatively and throughout the follow-up period, which lasted for at least one year.The Macnab efficacy criteria were used to assess postoperative outcomes during the final follow-up period.
Results: All patients successfully completed the 1-year follow-up on time. Two patients experienced postoperative wound liquefaction and successfully recovered after undergoing dressing changes. The average duration of the surgical procedure was 113.09 ± 6.97 min, and an intraoperative blood loss of 50.47 ± 21.32 millilitres was observed. Significant differences were noted in visual analog scale (VAS) scores before and after surgery at various time intervals, indicating improvement with the progression of rehabilitation exercises. No significant changes were found in the pelvic incidence (PI), and there were no notable differences between the preoperative and postoperative periods. No loosening, breakage, or failure of the internal fixation was found during the long-term follow-up. Furthermore, there were no serious complications, such as infection or vascular or nerve injuries. occurred during the procedure. A patient who presented with a considerable cryptic fissure of sacrum 1 experienced dural injury during the surgical procedure. Intraoperatively, dural sutures were skillfully applied, and the adjacent muscles were fortified. Remarkably, the patient achieved successful healing in a single stage. On the first day postsurgery, a gradual improvement in mobility was noted.
Conclusions: The use of a V-shaped titanium cable in conjunction with a pedicle screw internal fixation system for the management of fifth lumbar spondylolysis in young individuals is characterized by its ease of execution and ability to yield favorable outcomes. This approach relies on the prerequisite that patients with minimal intervertebral disc injury or mild lumbar spondylolisthesis demonstrate high overall success rates but experience low failure rates associated with internal fixation. Most significantly, this technique involves segmental internal fixation, which safeguards the functional spinal unit (FSU).
Keywords: Lumbar; Spondylolysis; V-type titanium cable system; Young adult.
© 2024. The Author(s).
Conflict of interest statement
Figures


Similar articles
-
[Effectiveness of U-shape titanium screw-rod fixation system with bone autografting for lumbar spondylolysis of young adults].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014 Mar;28(3):354-7. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2014. PMID: 24844019 Chinese.
-
Buck technique supplemented by temporary intersegmental pedicle screw fixation to repair lumbar spondylolysis in youth.J Orthop Surg Res. 2024 Jun 8;19(1):340. doi: 10.1186/s13018-024-04823-8. J Orthop Surg Res. 2024. PMID: 38849937 Free PMC article.
-
Minimally invasive unilateral pedicle screws and a translaminar facet screw fixation and interbody fusion for treatment of single-segment lower lumbar vertebral disease: surgical technique and preliminary clinical results.J Orthop Surg Res. 2017 Jul 20;12(1):117. doi: 10.1186/s13018-017-0606-z. J Orthop Surg Res. 2017. PMID: 28728587 Free PMC article. Clinical Trial.
-
[Clinical research progress of direct surgical repair of lumbar spondylolysis in young patients].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013 Jan;27(1):106-9. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2013. PMID: 23427504 Review. Chinese.
-
Double-level lumbar spondylolysis and spondylolisthesis: A retrospective study.J Orthop Surg Res. 2018 Mar 16;13(1):55. doi: 10.1186/s13018-018-0723-3. J Orthop Surg Res. 2018. PMID: 29548343 Free PMC article. Review.
References
-
- Chung CC, Shimer AL. Lumbosacral Spondylolysis and Spondylolisthesis. Clin Sports Med. 2021;40:471–90. - PubMed
-
- Sakai T, Sairyo K, Suzue N, Kosaka H, Yasui N. Incidence and etiology of lumbar spondylolysis: review of the literature. J Orthop Sci. 2010;15:281–8. - PubMed
-
- Fredrickson BE, Baker D, McHolick WJ, Yuan HA, Lubicky JP. The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am. 1984;66:699–707. - PubMed
-
- Debnath UK, Freeman BJC, Gregory P, de la Harpe D, Kerslake RW, Webb JK. Clinical outcome and return to sport after the surgical treatment of spondylolysis in young athletes. J Bone Joint Surg Br. 2003;85:244–9. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
