

Prospective pharmacotyping of urothelial carcinoma organoids for drug sensitivity prediction - feasibility and real world experience
- PMID: 39533373
- PMCID: PMC11558855
- DOI: 10.1186/s40164-024-00579-3
Prospective pharmacotyping of urothelial carcinoma organoids for drug sensitivity prediction - feasibility and real world experience
Abstract
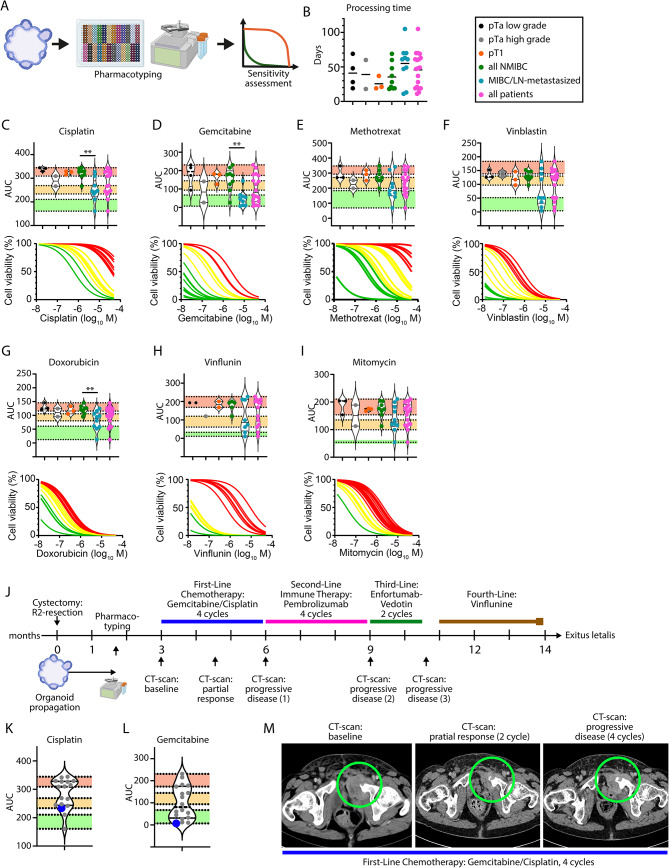
Urothelial carcinoma (UC) of the urinary bladder has significant challenges in treatment due to its diverse genetic landscape and variable response to systemic therapy. In recent years, patient-derived organoids (PDOs) emerged as a novel tool to model primary tumors with higher resemblance than conventional 2D cell culture approaches. However, the potential of organoids to predict therapy response in a clinical setting remains to be evaluated. This study explores the clinical feasibility of PDOs for pharmacotyping in UC. Initially, we subjected tumor tissue specimens from 50 patients undergoing transurethral resection or radical cystectomy to organoid propagation, of whom 19 (38%) yielded PDOs suitable for drug sensitivity assessment. Notably, whole transcriptome-based analysis indicated that PDOs may show phenotypes distinct from their parental tumor tissue. Pharmacotyping within a clinically relevant timeframe [mean of 35.44 and 55 days for non-muscle invasive bladder cancer (NMIBC) and muscle invasive bladder cancer (MIBC), respectively] was achieved. Drug sensitivity analyses revealed marked differences between NMIBC and MIBC, with MIBC-derived organoids demonstrating higher chemosensitivity toward clinically relevant drugs. A case study correlating organoid response with patient treatment outcome illustrated the complexity of predicting chemotherapy efficacy, especially considering the rapid acquisition of drug resistance. We propose a workflow of prospective organoid-based pharmacotyping in UC, enabling further translational research and integration of this approach into clinical practice.
Keywords: Patient-derived organoids; Pharmacotyping; Urothelial carcinoma.
© 2024. The Author(s).
Conflict of interest statement
Figures

References
-
- Babjuk M, et al. European Association of Urology Guidelines on non–muscle-invasive bladder Cancer (Ta, T1, and carcinoma in situ). Eur Urol. 2022;81:75–94. 10.1016/j.eururo.2021.08.010. - PubMed
-
- Alfred Witjes J, et al. European Association of Urology Guidelines on muscle-invasive and metastatic bladder Cancer: Summary of the 2023 guidelines. Eur Urol. 2023. 10.1016/j.eururo.2023.08.016. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
