

Prognostic nomograms for locally advanced cervical cancer based on the SEER database: Integrating Cox regression and competing risk analysis
- PMID: 39533612
- PMCID: PMC11557032
- DOI: 10.1097/MD.0000000000040408
Prognostic nomograms for locally advanced cervical cancer based on the SEER database: Integrating Cox regression and competing risk analysis
Abstract
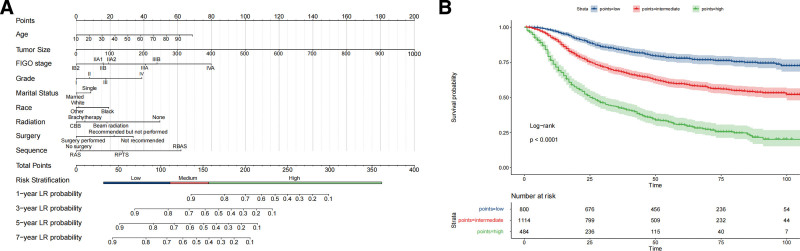
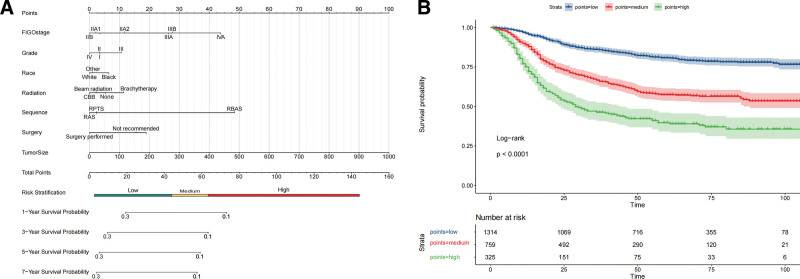
Locally advanced cervical carcinoma (LACC) remains a significant global health challenge owing to its high recurrence rates and poor outcomes, despite current treatments. This study aimed to develop a comprehensive risk stratification model for LACC by integrating Cox regression and competing risk analyses. This was done to improve clinical decision making. We analyzed data from 3428 patients with LACC registered in the Surveillance, Epidemiology, and End Results program and diagnosed them between 2010 and 2015. Cox regression and competing risk analyses were used to identify the prognostic factors. We constructed and validated nomograms for overall survival (OS) and disease-specific survival (DSS). Multivariate Cox regression identified key prognostic factors for OS, including advanced International Federation of Gynecology and Obstetrics stage, age, marital status, ethnicity, and tumor size. Notably, International Federation of Gynecology and Obstetrics stages IIIA, IIIB, and IVA had hazard ratios of 2.227, 2.451, and 4.852, respectively, significantly increasing the mortality risk compared to stage IB2. Ethnic disparities were evident, with African Americans facing a 39.8% higher risk than Caucasians did. Competing risk analyses confirmed the significance of these factors in DSS, particularly tumor size. Our nomogram demonstrated high predictive accuracy, with area under the curve values ranging from 0.706 to 0.784 for DSS and 0.717 to 0.781 for OS. Calibration plots and decision curve analyses further validated the clinical utility of this nomogram. We present effective nomograms for LACC risk stratification that incorporate multiple prognostic factors. These models provide a refined approach for individualized patient management and have the potential to significantly enhance therapeutic strategies for LACC.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
[Establishment of a prognostic nomogram and discussion on optimal treatment for cervical adenocarcinoma:a retrospective study based on SEER database and Chinese single-center data].Zhonghua Fu Chan Ke Za Zhi. 2024 Apr 25;59(4):307-319. doi: 10.3760/cma.j.cn112141-20231101-00172. Zhonghua Fu Chan Ke Za Zhi. 2024. PMID: 38644277 Chinese.
-
Nomogram for Predicting Survival in Locally Advanced Cervical Cancer with Concurrent Chemoradiotherapy plus or Not Adjuvant Chemotherapy: A Retrospective Analysis Based on 2018 FIGO Staging.Cancer Biother Radiopharm. 2024 Nov;39(9):690-705. doi: 10.1089/cbr.2023.0199. Epub 2024 Jun 3. Cancer Biother Radiopharm. 2024. PMID: 38828494
-
Nomograms predicting the overall survival and cancer-specific survival of patients with stage IIIC1 cervical cancer.BMC Cancer. 2021 Apr 23;21(1):450. doi: 10.1186/s12885-021-08209-5. BMC Cancer. 2021. PMID: 33892663 Free PMC article.
-
Competing risk nomogram and risk classification system for evaluating overall and cancer-specific survival in neuroendocrine carcinoma of the cervix: a population-based retrospective study.J Endocrinol Invest. 2024 Jun;47(6):1545-1557. doi: 10.1007/s40618-023-02261-7. Epub 2024 Jan 3. J Endocrinol Invest. 2024. PMID: 38170396 Free PMC article.
-
Proportions and incidence of locally advanced cervical cancer: a global systematic literature review.Int J Gynecol Cancer. 2022 Dec 5;32(12):1531-1539. doi: 10.1136/ijgc-2022-003801. Int J Gynecol Cancer. 2022. PMID: 36241221 Free PMC article.
Cited by
-
Prognostic value of circ_0000043/miR-590-5p in cervical cancer and regulation of tumor progression.Discov Oncol. 2025 May 23;16(1):879. doi: 10.1007/s12672-025-02670-5. Discov Oncol. 2025. PMID: 40407961 Free PMC article.
References
-
- Cohen PA, Jhingran A, Oaknin A, Denny L. Cervical cancer. Lancet. 2019;393:169–82. - PubMed
-
- Abu-Rustum NR, Yashar CM, Bean S, et al. . NCCN guidelines insights: cervical cancer, version 1.2020. J Natl Compr Canc Netw. 2020;18:660–6. - PubMed
-
- Dyer BA, Zamarin D, Eskandar RN, Mayadev JM. Role of immunotherapy in the management of locally advanced and recurrent/metastatic cervical cancer. J Natl Compr Canc Netw. 2019;17:91–7. - PubMed
