

Impact of Different Angiotensin-Converting Enzyme Inhibitors or Angiotensin Receptor Blocker Resumption Timing on Post Acute Kidney Injury Outcomes
- PMID: 39534209
- PMCID: PMC11551097
- DOI: 10.1016/j.ekir.2024.08.027
Impact of Different Angiotensin-Converting Enzyme Inhibitors or Angiotensin Receptor Blocker Resumption Timing on Post Acute Kidney Injury Outcomes
Abstract
Introduction: Evidence suggests a survival benefit from resuming angiotensin-converting enzyme inhibitors (ACEI) or angiotensin receptor blockers (ARB) post acute kidney injury (AKI) compared to nonuse; however, the optimal timing and its impact on outcomes are unclear. The risks of earlier resumption, such as recurrent AKI or hyperkalemia, remain unexplored.
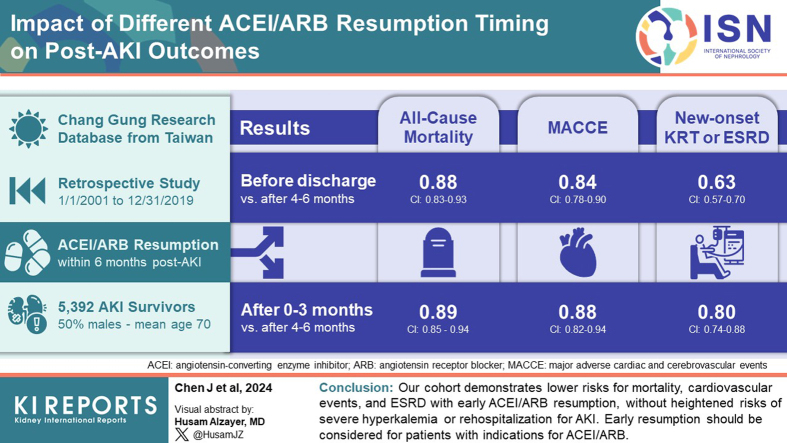
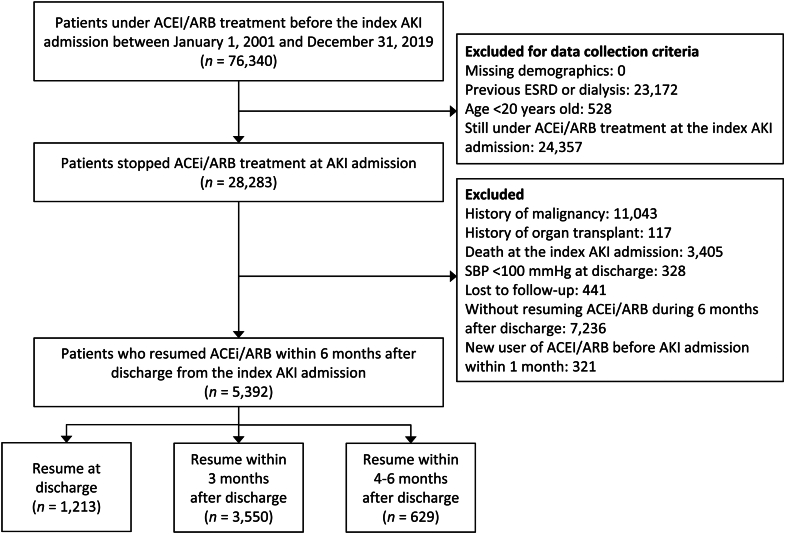
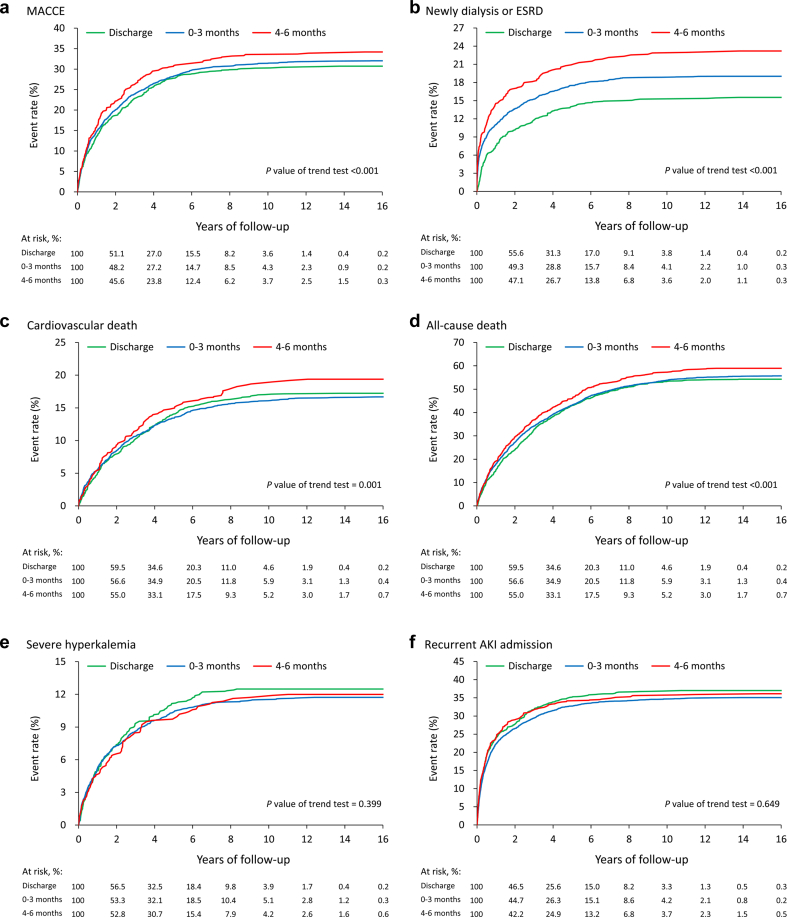
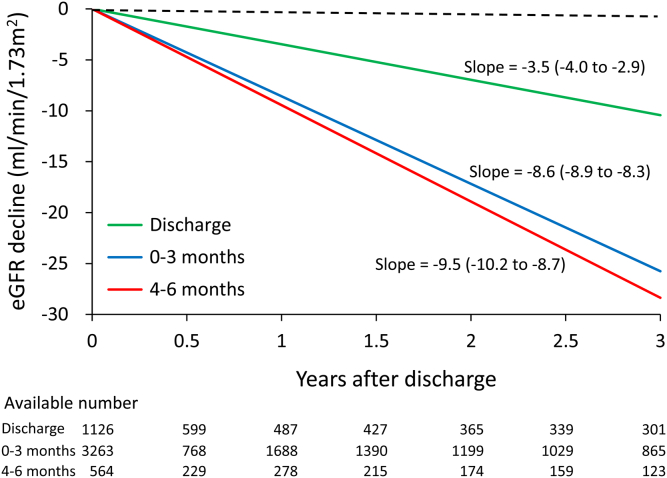
Methods: Using multiinstitutional electronic health records, we analyzed the relationship between 3 ACEI or ARB (ACEI/ARB) resumption timelines post-AKI (prior to discharge, 0-3 months, and 4-6 months postdischarge) and outcomes including all-cause mortality, major adverse cardiac and cerebrovascular events (MACCEs), dialysis initiation or end-stage renal disease (ESRD), severe hyperkalemia, and recurrent AKI with hospitalization. Cox proportional models estimated hazard ratios (HRs) for outcomes across different resumption timings, following a target trial design.
Results: Among 5392 AKI survivors resuming ACEI/ARB within 6 months post-AKI, earlier resumption was associated with lower mortality, MACCE, MACCE-related mortality, new dialysis initiation or ESRD (P < 0.001 in trend tests), without increased risks of severe hyperkalemia and re-AKI admissions. Early resumption has a lower mortality compared to 4 to 6 months postdischarge (before discharge, HR: 0.88, 95% confidence interval [CI]: 0.83-0.93; 0-3 months, HR: 0.89, 95% CI: 0.85-0.94). Subgroup analysis showed a lower mortality HR from earlier resumption among AKI survivors with prior ACEI/ARB comorbidity indications (P < 0.001 in trend tests; before discharge, HR: 0.85, 95% CI: 0.80-0.90; 0-3 months, HR: 0.88, 95% CI: 0.83-0.93).
Conclusion: Our cohort demonstrates lower risks for mortality, cardiovascular events, and ESRD with early ACEI/ARB resumption, without heightened risks of severe hyperkalemia or rehospitalization for AKI. Early resumption should be considered for patients with indications for ACEI/ARB.
Keywords: ACEI; ARB; RAAs inhibitor; acute kidney disease; acute kidney injury; resumption.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
Similar articles
-
Effect of Post-Acute Kidney Injury Use of Renin-Angiotensin Inhibitors on Long-term Mortality and Major Adverse Kidney Events: A 5-year Retrospective Observational Cohort Study.Kidney Med. 2025 Mar 20;7(5):100996. doi: 10.1016/j.xkme.2025.100996. eCollection 2025 May. Kidney Med. 2025. PMID: 40321973 Free PMC article.
-
The Impact of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers on Clinical Outcomes of Acute Kidney Disease Patients: A Systematic Review and Meta-Analysis.Front Pharmacol. 2021 Jul 20;12:665250. doi: 10.3389/fphar.2021.665250. eCollection 2021. Front Pharmacol. 2021. PMID: 34354583 Free PMC article. Review.
-
Association of Angiotensin-Converting Enzyme Inhibitor or Angiotensin Receptor Blocker Use With Outcomes After Acute Kidney Injury.JAMA Intern Med. 2018 Dec 1;178(12):1681-1690. doi: 10.1001/jamainternmed.2018.4749. JAMA Intern Med. 2018. PMID: 30422153 Free PMC article.
-
Stopping renin-angiotensin system blockers after acute kidney injury and risk of adverse outcomes: parallel population-based cohort studies in English and Swedish routine care.BMC Med. 2020 Jul 29;18(1):195. doi: 10.1186/s12916-020-01659-x. BMC Med. 2020. PMID: 32723383 Free PMC article.
-
The association between dual RAAS inhibition and risk of acute kidney injury and hyperkalemia in patients with diabetic kidney disease: a systematic review and meta-analysis.Nephrol Dial Transplant. 2023 Oct 31;38(11):2503-2516. doi: 10.1093/ndt/gfad101. Nephrol Dial Transplant. 2023. PMID: 37309038 Free PMC article.
Cited by
-
The burden of acute kidney disease: an epidemiological review and importance of follow-up care.Clin Kidney J. 2025 May 27;18(6):sfaf169. doi: 10.1093/ckj/sfaf169. eCollection 2025 Jun. Clin Kidney J. 2025. PMID: 40599626 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
