

Using machine learning to predict neurologic injury in venovenous extracorporeal membrane oxygenation recipients: An ELSO Registry analysis
- PMID: 39534333
- PMCID: PMC11551311
- DOI: 10.1016/j.xjon.2024.06.013
Using machine learning to predict neurologic injury in venovenous extracorporeal membrane oxygenation recipients: An ELSO Registry analysis
Abstract
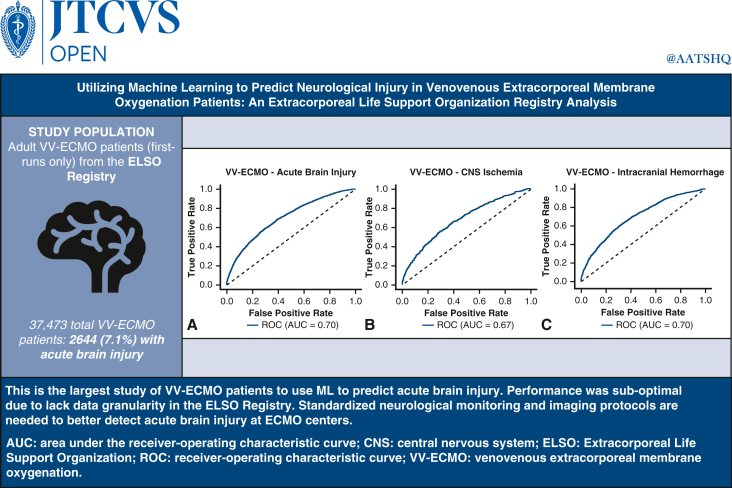
Background: Venovenous extracorporeal membrane oxygenation (VV-ECMO) is associated with acute brain injury (ABI), including central nervous system (CNS) ischemia (defined as ischemic stroke or hypoxic-ischemic brain injury [HIBI]) and intracranial hemorrhage (ICH). Data on prediction models for neurologic outcomes in VV-ECMO are limited.
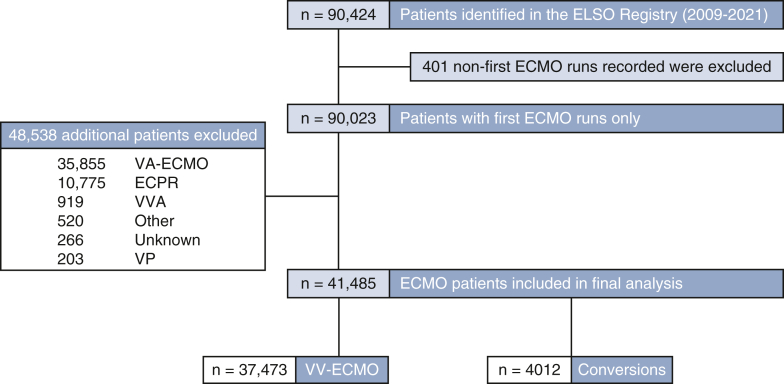
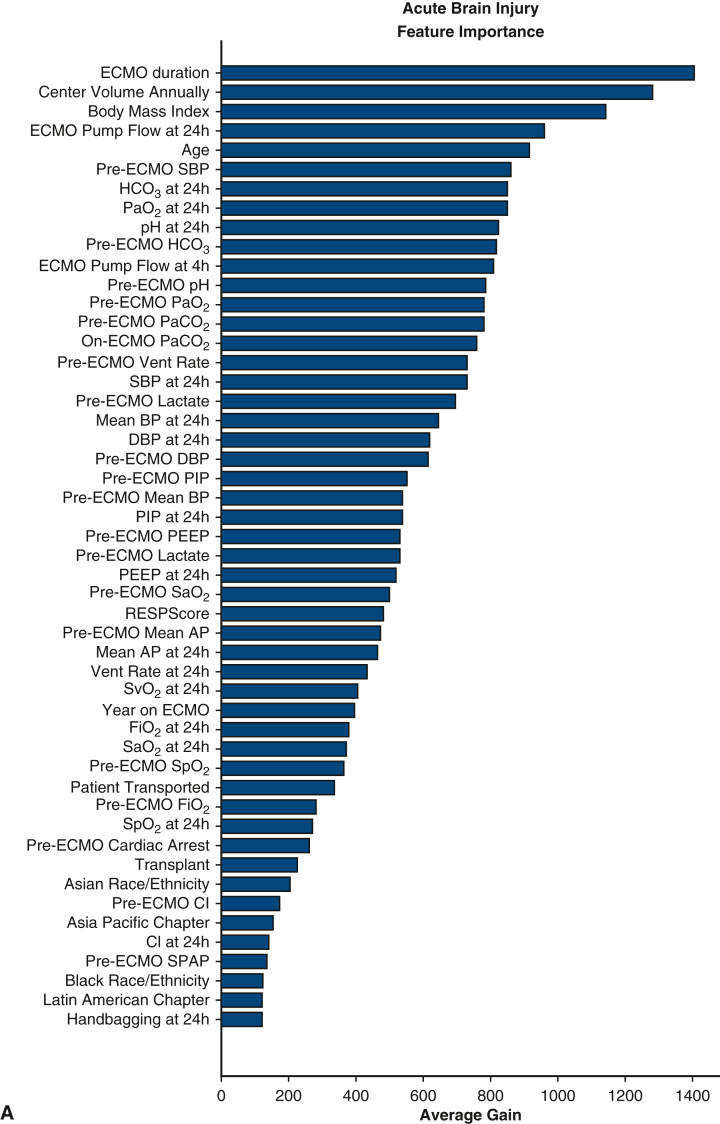
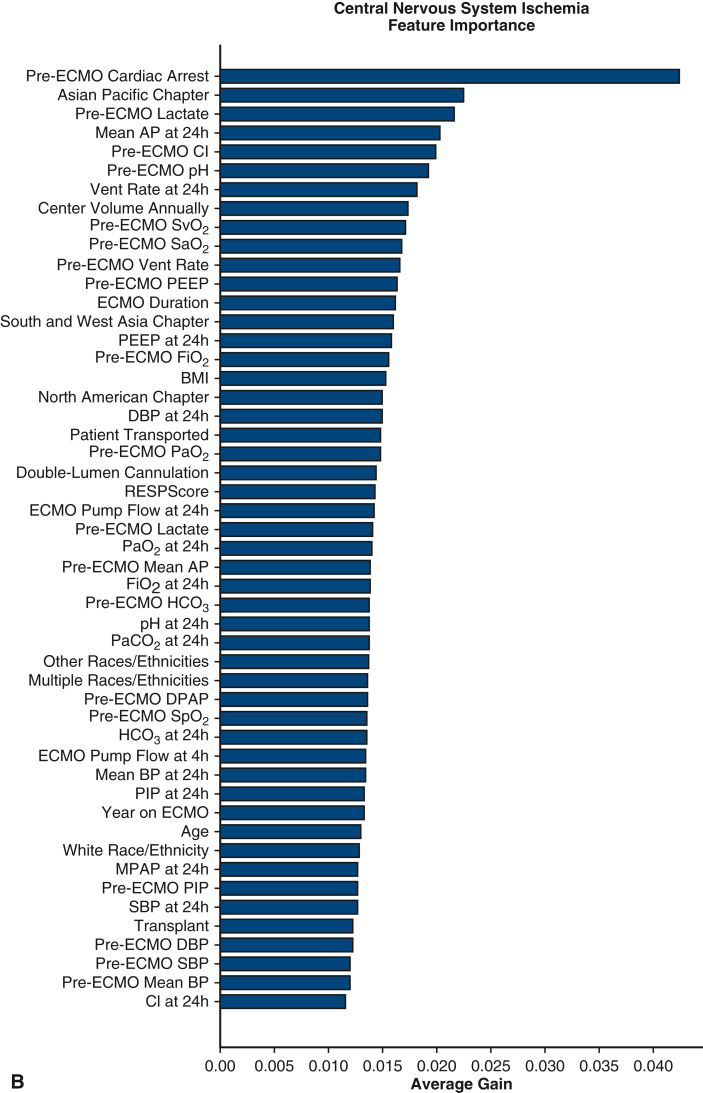
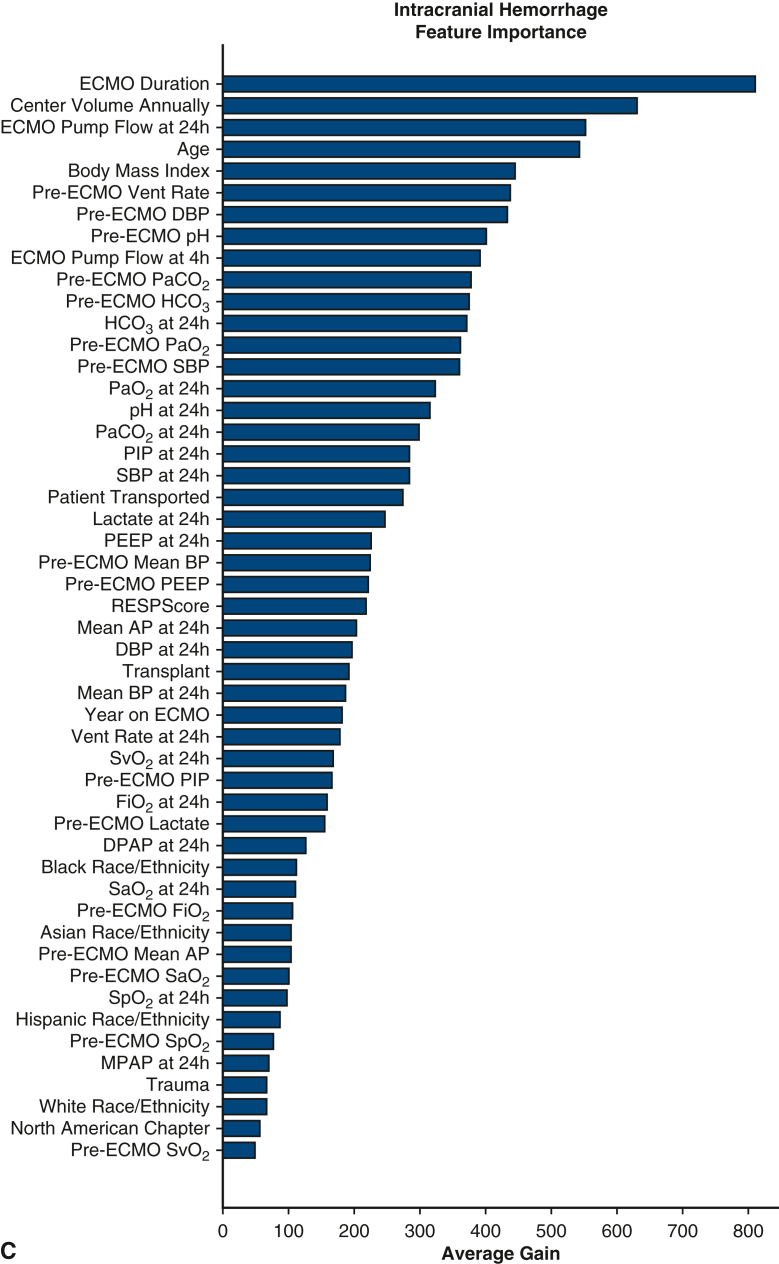
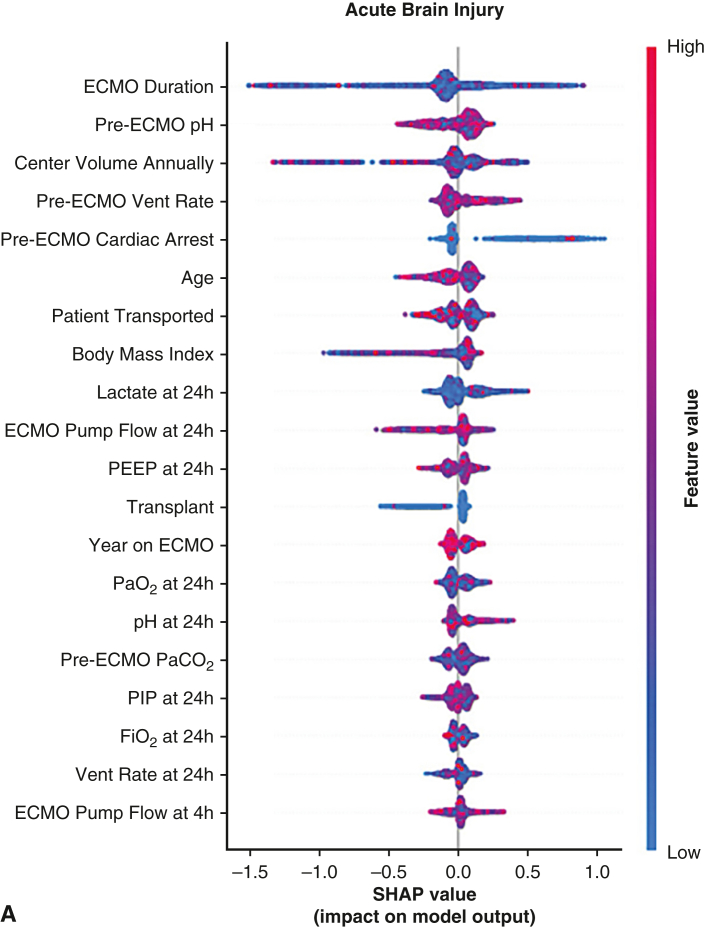
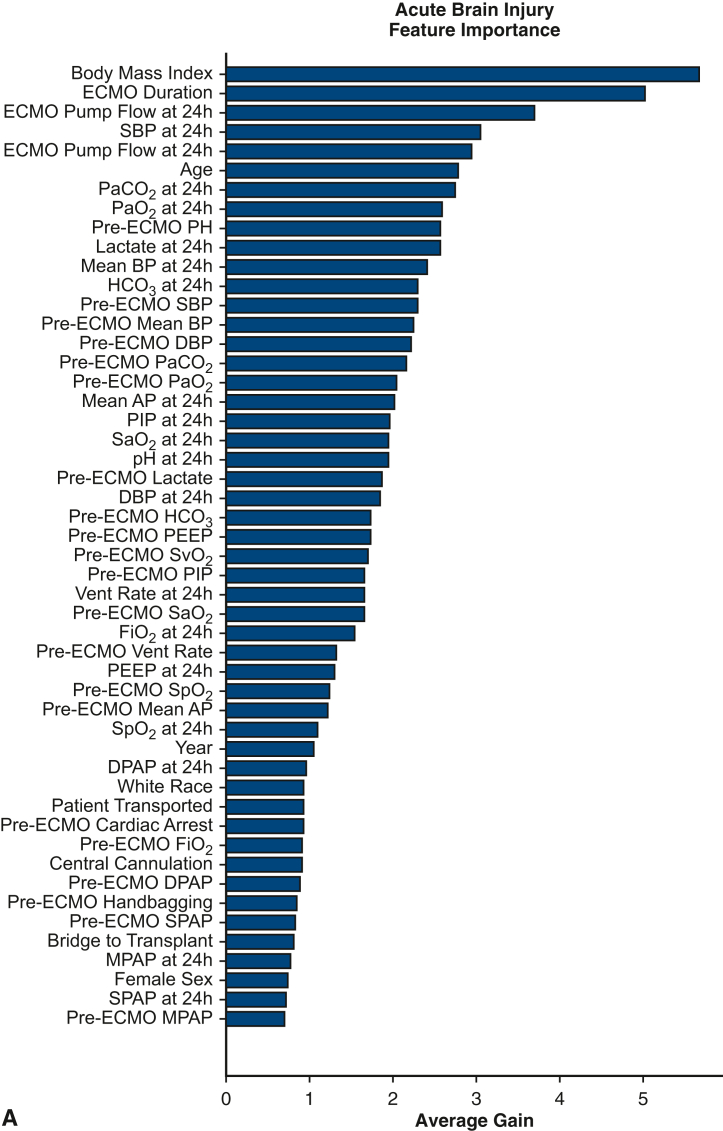
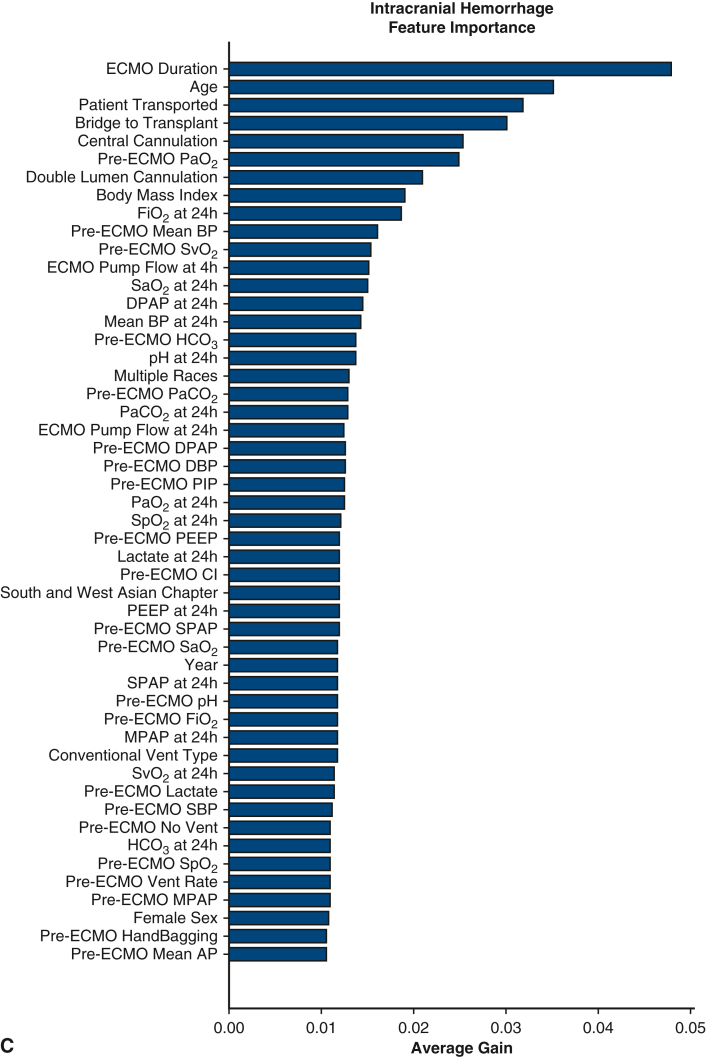
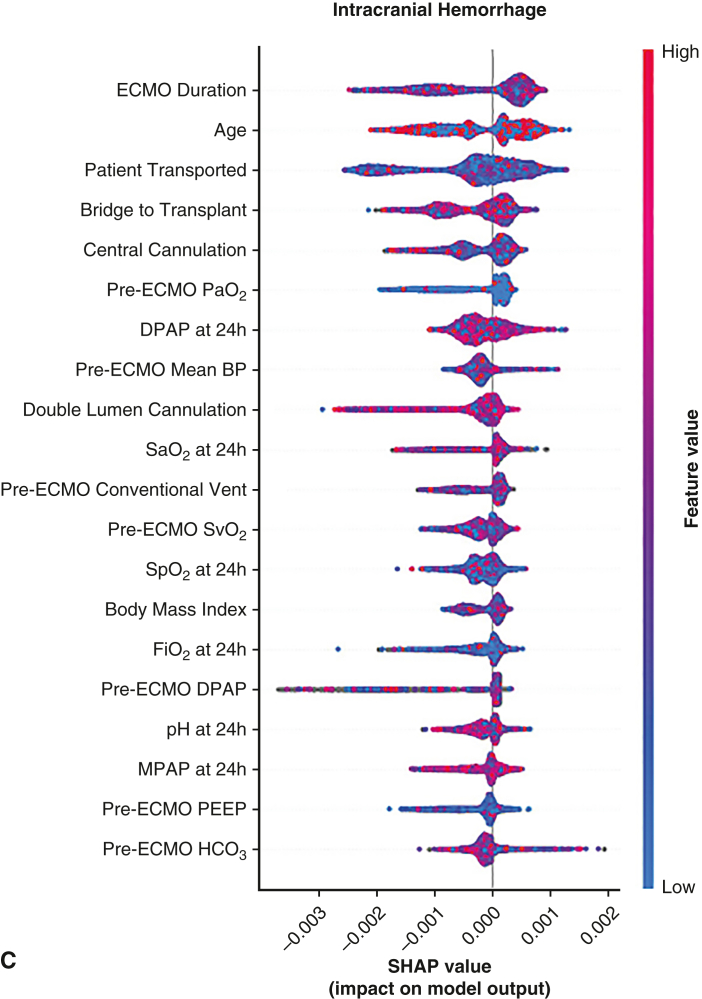
Methods: We analyzed adult (age ≥18 years) VV-ECMO patients in the Extracorporeal Life Support Organization (ELSO) Registry (2009-2021) from 676 centers. ABI was defined as CNS ischemia, ICH, brain death, and seizures. Data on 67 variables were extracted, including clinical characteristics and pre-ECMO/on-ECMO variables. Random forest, CatBoost, LightGBM, and XGBoost machine learning (ML) algorithms (10-fold leave-one-out cross-validation) were used to predict ABI. Feature importance scores were used to pinpoint the most important variables for predicting ABI.
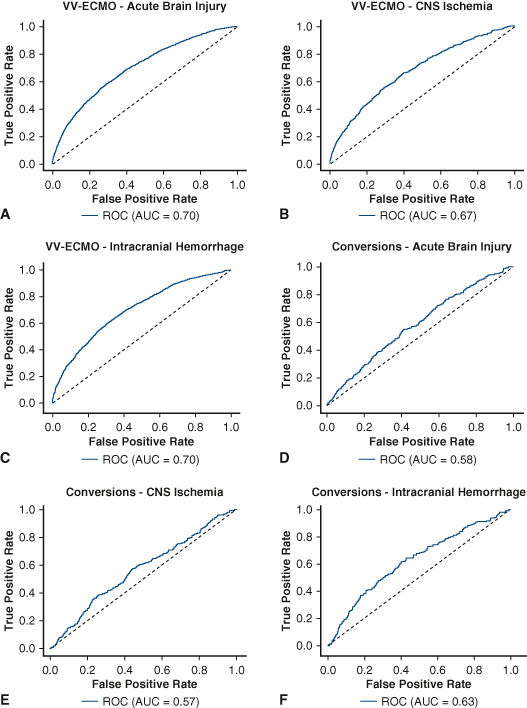
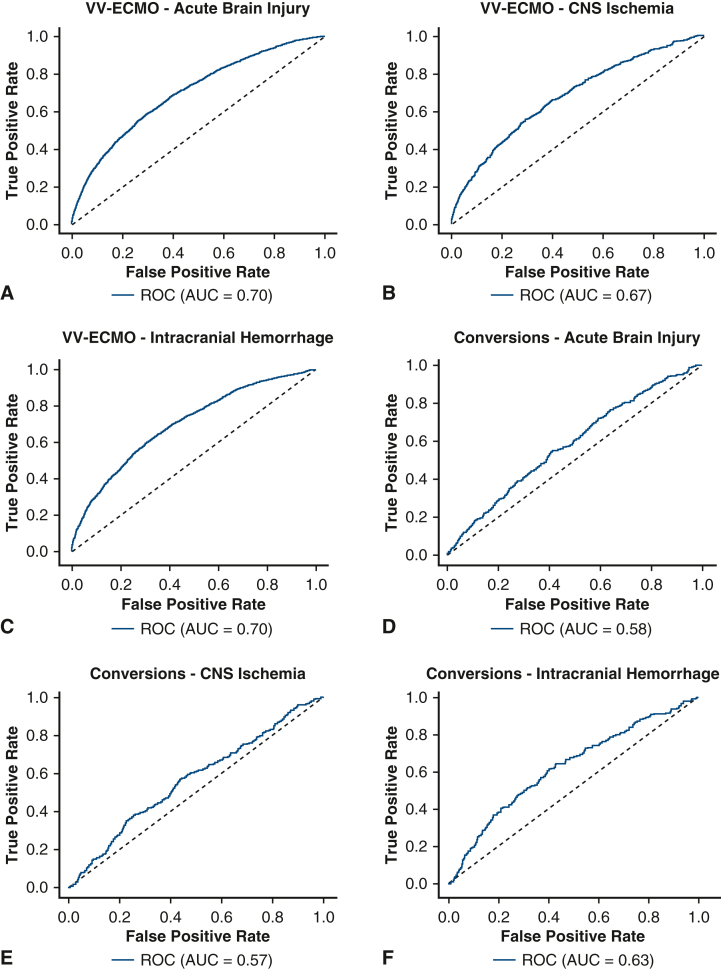
Results: Of 37,473 VV-ECMO patients (median age, 48.1 years; 63% male), 2644 (7.1%) experienced ABI, including 610 (2%) with CNS ischemia and 1591 (4%) with ICH. The areas under the receiver operating characteristic curve for predicting ABI, CNS ischemia, and ICH were 0.70, 0.68, and 0.70, respectively. The accuracy, positive predictive value, and negative predictive value for ABI were 85%, 19%, and 95%, respectively. ML identified higher center volume, pre-ECMO cardiac arrest, higher ECMO pump flow, and elevated on-ECMO serum lactate level as the most important risk factors for ABI and its subtypes.
Conclusions: This is the largest study of VV-ECMO patients to use ML to predict ABI reported to date. Performance was suboptimal, likely due to lack of standardization of neuromonitoring/imaging protocols and data granularity in the ELSO Registry. Standardized neurologic monitoring and imaging are needed across ELSO centers to detect the true prevalence of ABI.
Keywords: acute brain injury; machine learning; neurologic complications; venovenous extracorporeal membrane oxygenation.
© 2024 The Author(s).
Conflict of interest statement
Dr Brodie receives research support from and consults for LivaNova. He has been on the medical advisory boards for Xenios, Medtronic, Inspira and Cellenkos. He is the President-elect of ELSO and the Chair of the Executive Committee of the International ECMO Network (ECMONet), and he writes for UpToDate. Dr Ventetuolo has been a consultant or served on advisory boards for Merck, Janssen, and Regeneron outside of the submitted work. Sung-Min Cho is supported by the National Heart, Lung and Blood Institute (1K23HL157610) and Hyperfine (SAFE MRI ECMO study). All other authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures







References
-
- Cho S.M., Canner J., Caturegli G., et al. Risk factors of ischemic and hemorrhagic strokes during venovenous extracorporeal membrane oxygenation: analysis of data from the extracorporeal life support organization registry. Crit Care Med. 2021;49(1):91–101. doi: 10.1097/ccm.0000000000004707. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
