

Importance of surgeon's experience in practicing valve-sparing aortic root replacement
- PMID: 39534352
- PMCID: PMC11551295
- DOI: 10.1016/j.xjon.2024.07.013
Importance of surgeon's experience in practicing valve-sparing aortic root replacement
Abstract
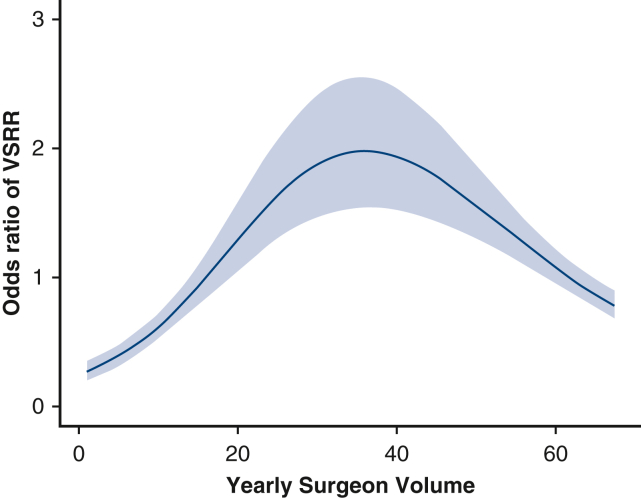
Background: Valve-sparing root replacement (VSRR) requires a unique skill set. This study aimed to examine the influence of surgeon's procedural volume on outcomes of VSRR.
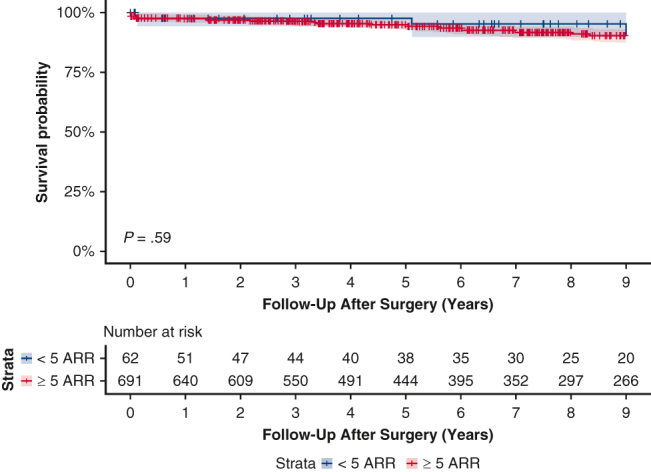
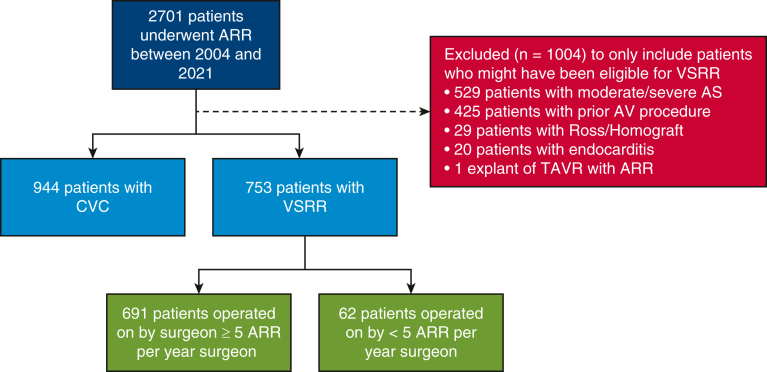
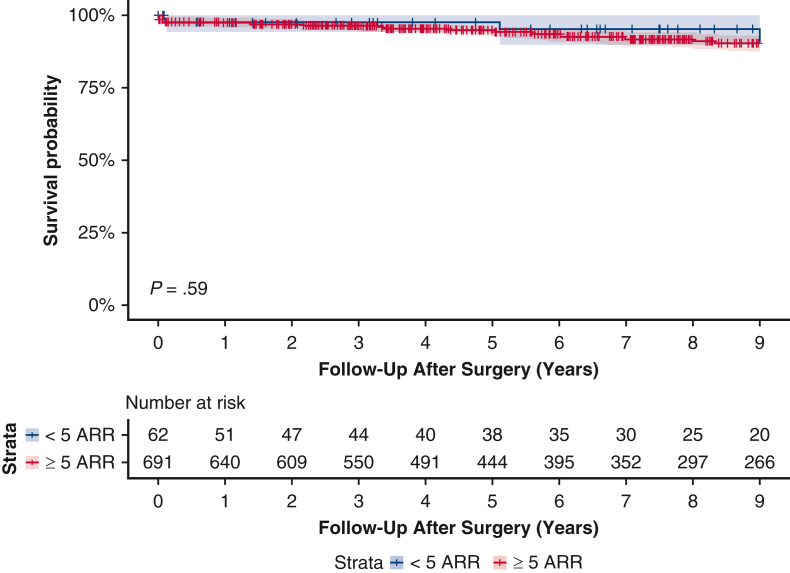
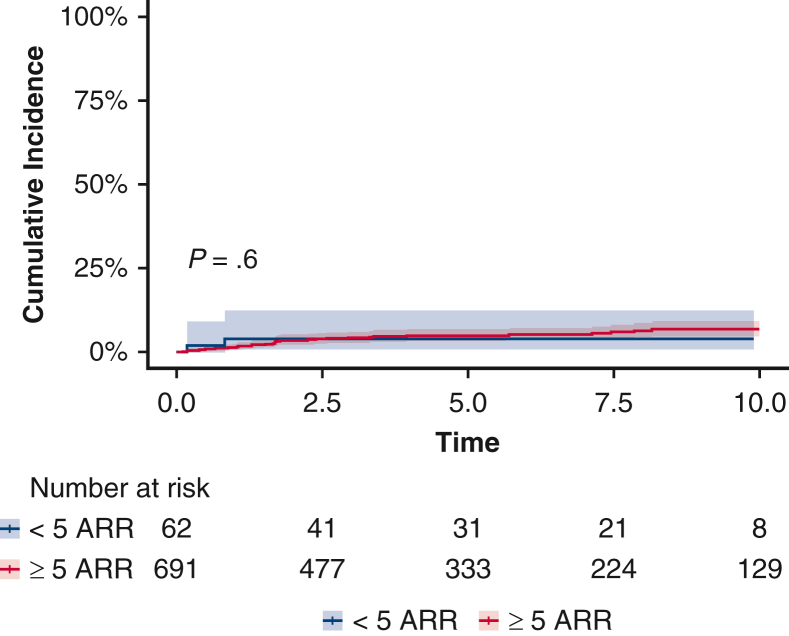
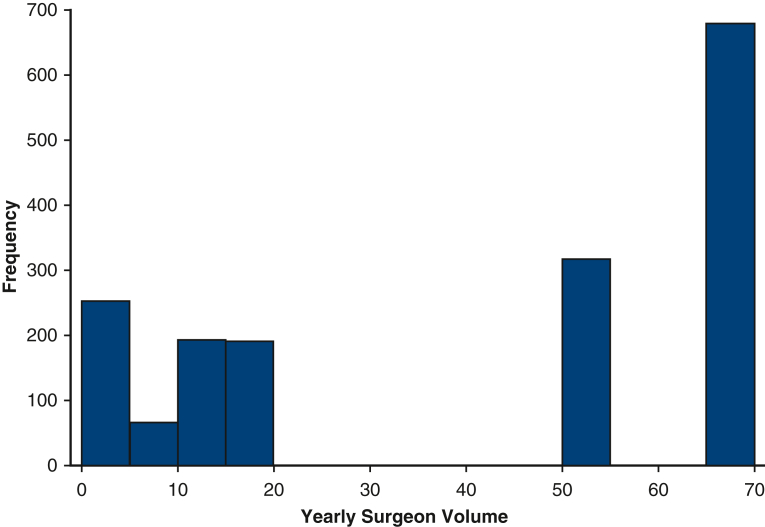
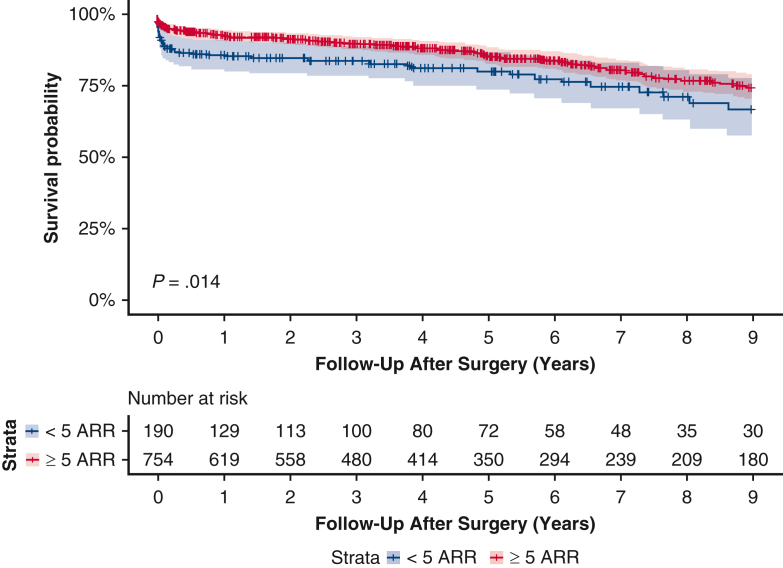
Methods: This retrospective study included 1697 patients from 2 large, high-volume aortic centers who underwent aortic root replacement (ARR) between 2004 and 2021 and were potentially eligible for VSRR. Surgeons were classified as performing <5 ARRs or ≥5 ARRs annually. Multivariable logistic regression was used to examine the independent association of surgeon volume and the decision to perform VSRR. Inverse probability treatment weighting (IPTW) was used to match patients who were operated on by <5 ARR surgeons or ≥5 ARR surgeons and compare long-term survival probability. Cumulative incidence curves with mortality as a competing risk were plotted to compare the rate of aortic valve reoperation.
Results: Of 1697 patients who met the study inclusion criteria, 944 underwent composite-valve conduit ARR and 753 underwent VSRR. The median age of the cohort was 57 years (interquartile range, 45-66 years), and 268 (15.8%) were female. Aortic insufficiency was present in 1105 patients (65.1%), and 200 of the procedures (11.8%) were reoperations. The indication for surgery was aneurysm in 1496 patients (88.2%) and dissection in 201 (11.8%). Among the 743 patients who underwent VSRR, 691 (92%) were operated on by ≥ 5 ARR surgeons and 62 (8%) were operated on by <5 ARR surgeons. In multivariable logistic regression, ≥5 ARRs (odds ratio, 3.33; 95% confidence interval, 2.34-4.73; P < .001) was associated with VSRR as the procedure of choice. Following IPTW, there was no significant difference between <5 ARR and ≥5 ARR surgeons in survival probability after VSRR (P = .59) or in the rate of aortic valve reoperation (P = .60).
Conclusions: In the setting of a high-volume aortic center, patients who undergo ARR are less likely to receive VSRR if operated on by a <5 ARR surgeon; however, VSRR may be safely performed by <5 ARR surgeons.
Keywords: aortic root replacement; inverse probability treatment weighting; surgeon volume; valve-sparing root replacement.
© 2024 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures
Similar articles
-
A multicentre, propensity score matched analysis comparing a valve-sparing approach to valve replacement in aortic root aneurysm: Insight from the AVIATOR database.Eur J Cardiothorac Surg. 2023 Feb 3;63(2):ezac514. doi: 10.1093/ejcts/ezac514. Eur J Cardiothorac Surg. 2023. PMID: 36308450 Free PMC article.
-
Valve-Sparing vs Bio-Bentall Aortic Root Replacement in Patients Aged 60 to 75 Years: Survival, Reintervention, and Aortic Regurgitation.Ann Thorac Surg. 2025 May;119(5):990-999. doi: 10.1016/j.athoracsur.2024.12.028. Epub 2025 Jan 17. Ann Thorac Surg. 2025. PMID: 39828076
-
Aortic valve-sparing operation at concomitant aortic root and total aortic arch replacement.Gen Thorac Cardiovasc Surg. 2025 Apr 23. doi: 10.1007/s11748-025-02150-1. Online ahead of print. Gen Thorac Cardiovasc Surg. 2025. PMID: 40266547
-
Comparing outcomes between valve-sparing root replacement and the Bentall procedure in proximal aortic aneurysms: systematic review and meta-analysis.Interact Cardiovasc Thorac Surg. 2019 Dec 1;29(6):911-922. doi: 10.1093/icvts/ivz211. Interact Cardiovasc Thorac Surg. 2019. PMID: 31504555
-
Is valve-sparing root replacement a safe option in acute type A aortic dissection? A systematic review and meta-analysis.Interact Cardiovasc Thorac Surg. 2019 Nov 1;29(5):766-775. doi: 10.1093/icvts/ivz180. Interact Cardiovasc Thorac Surg. 2019. PMID: 31365078
References
-
- Nishimura R.A., Otto C.M., Bonow R.O., et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135:e1159–e1195. doi: 10.1161/CIR.0000000000000503. - DOI - PubMed
-
- Ommen S.R., Mital S., Burke M.A., et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical Practice Guidelines. J Am Coll Cardiol. 2020;76(25):3022–3055. doi: 10.1016/j.jacc.2020.08.044. - DOI - PubMed
-
- Kim L.K., Swaminathan R.V., Looser P., et al. Hospital volume outcomes after septal myectomy and alcohol septal ablation for treatment of obstructive hypertrophic cardiomyopathy: US nationwide inpatient database, 2003-2011. JAMA Cardiol. 2016;1(3):324–332. doi: 10.1001/jamacardio.2016.0252. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
