

Prognostic risk and survival of asymptomatic IgM monoclonal gammopathy: Results from a Spanish Multicenter Registry
- PMID: 39534383
- PMCID: PMC11555297
- DOI: 10.1002/hem3.70029
Prognostic risk and survival of asymptomatic IgM monoclonal gammopathy: Results from a Spanish Multicenter Registry
Abstract
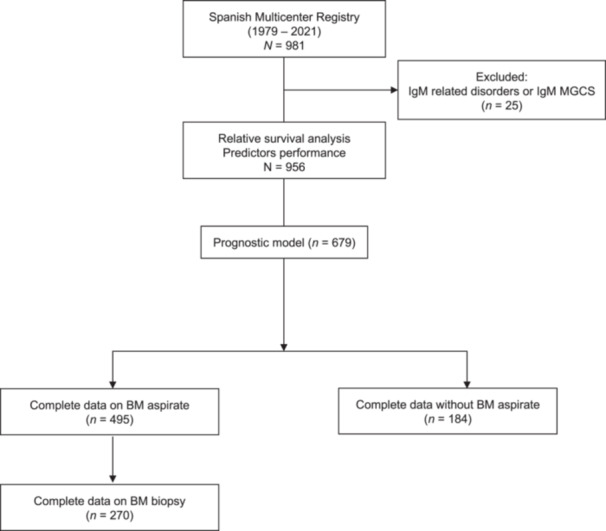
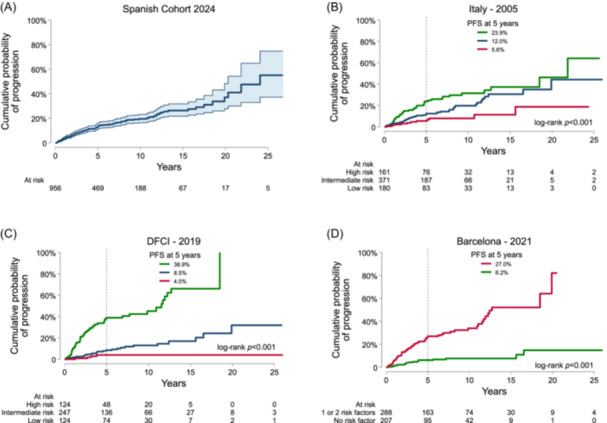
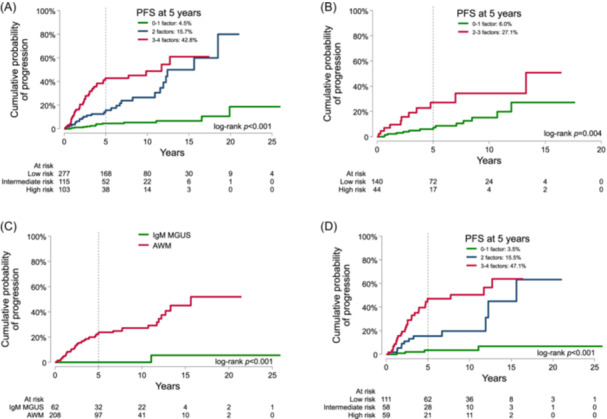
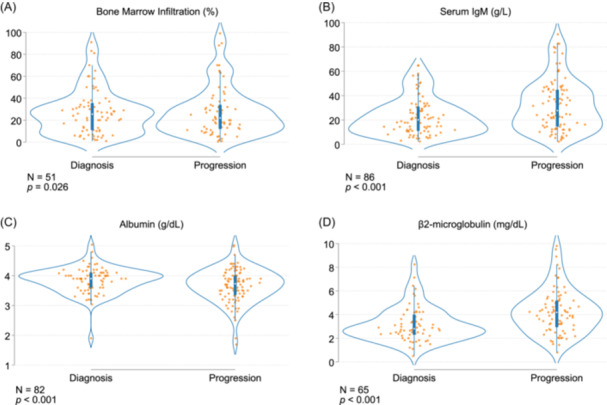
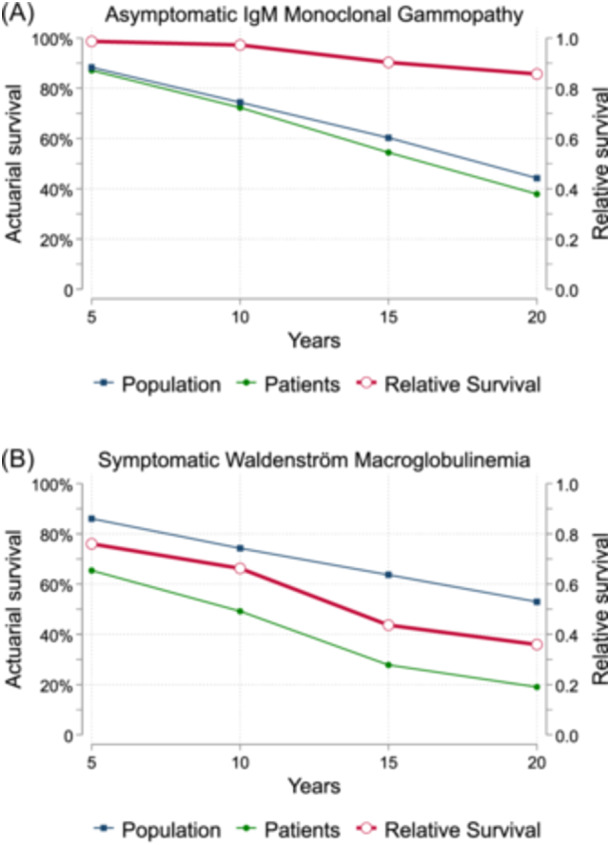
Asymptomatic IgM gammopathy encompasses IgM monoclonal gammopathy of undetermined significance (MGUS) and asymptomatic Waldenström macroglobulinemia (AWM), both having a risk of progression to symptomatic disease. Here, we assessed the risk of progression and the mortality of 956 patients with asymptomatic IgM gammopathy across 25 Spanish centers. After a median follow-up of 5.7 years, 156 patients progressed, most of them to symptomatic WM (SWM). The cumulative incidence of progression was 13% and 20% at 5 and 10 years, respectively. The serum IgM ≥10 g/L, bone marrow (BM) infiltration ≥20%, β2-microglobulin ≥3 mg/L, and albumin <4 g/dL were the most potent predictors of disease progression in a multivariate Cox regression model, allowing the identification of three risk categories. The probability of progression to symptomatic disease at 5 years was 4.5%, 15.7%, and 42.8% for low-, intermediate-, and high-risk groups, respectively. In patients without a BM evaluation, the presence of none or 1 risk factor and 2 or 3 risk factors conferred a progression risk of 6% and 27% at 5 years, respectively. The model was independent of the presence of MYD88 L265P, which conferred a negative impact only in AWM patients. The relative survival (RS) ratio at 5 years of asymptomatic patients was similar to the Spanish population, which contrasted with the 0.76 5-year RS of SWM patients. Overall, the Spanish Multicenter Model comprehensively describes the risk of progression of asymptomatic patients and shows that the excess mortality is increased only in the symptomatic stage of the disease.
© 2024 The Author(s). HemaSphere published by John Wiley & Sons Ltd on behalf of European Hematology Association.
Conflict of interest statement
David F. Moreno received travel grants and honoraria from Janssen. Carlos Fernández de Larrea consulted and received honoraria from GSK, Sanofi, Pfizer, BeiGene, Amgen, BMS, and Janssen and received research funding from GSK, Amgen, and Janssen. Mario Arnao consulted and was on the speakers bureau for Janssen, Sanofi, and Amgen and consulted for BMS/Celgene. Ángela Heredia was on the speakers bureau for Janssen and NovoNordisk. Ricarda García‐Sánchez was on the speakers bureau and consulted for BMS/Celgene, Janssen‐Cilag, and GSK; consulted for Amgen and Takeda; and was on the advisory board member for Janssen‐Cilag, BMS/Celgene, Amgen, GSK, Takeda, and Beigene. Pablo Ríos Rull consulted, received honoraria, and was on the speakers bureau for GSK, AMGEN, and Sanofi; received honoraria from Celgene and Takeda; consulted for Beigene; has participated in medical meetings for GSK, Janssen, Celgene, Takeda, Amgen, Novartis, and Sanofi; and received research funding from BMS/Celgene. Ramón García‐Sanz received research support from the Asociación Española Contra el Cáncer, Takeda, Gilead, Incyte, Janssen; received honoraria from Beigene, Amgen, Takeda, Janssen, Incyte, BMS; and was on the speakers bureau for Beigene, Takeda, Janssen. Fernando Escalante consulted for Janssen Oncology, Amgen, GlaxoSmithKline, BeiGene, Sanofi; was on the speakers bureau for Janssen Oncology, GlaxoSmithKline; and received travel grants from BeiGene, Janssen Oncology, Amgen. Miguel Á. Canales consulted for Beigene, BMS, Incyte, Janssen, Karyopharm, Kite, Kyowa, Lilly, Roche, Takeda; and was part of the speakers bureau for Incyte, Janssen, Kite, Kyowa, Roche, Takeda. Luis Palomera received honoraria for lectures and advisory boards from Janssen, Amgen, Sanofi, GSK. The remaining authors declare no competing conflicts of interests.
Figures
References
LinkOut - more resources
Full Text Sources