

Discrepancy Rates in Acute Abdominal CT: An Audit of In-House and Remote Reporting Compared to Intraoperative Laparoscopic and Laparotomy Findings
- PMID: 39534545
- PMCID: PMC11555757
- DOI: 10.7759/cureus.73509
Discrepancy Rates in Acute Abdominal CT: An Audit of In-House and Remote Reporting Compared to Intraoperative Laparoscopic and Laparotomy Findings
Abstract
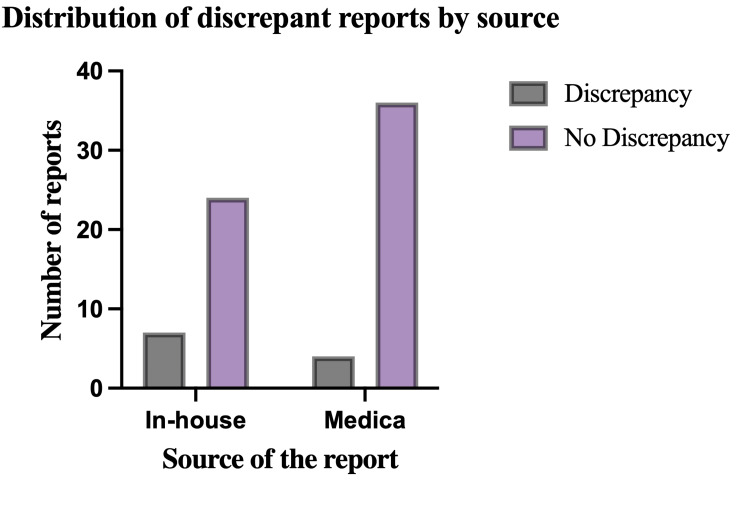
Introduction: Non-traumatic abdominal pain is a common emergency presentation frequently managed by general surgeons. Abdominopelvic computed tomography (CT) scans are the most popular imaging modality in this context. In many hospitals, the rising demand for urgent and emergent scans out-of-hours has necessitated the outsourcing of this service to teleradiology companies, whereby reports are generated at sites remote from the image acquisition. The primary aim of this study was to determine the discrepancy rates of preoperative CT imaging by source (teleradiology compared to in-house).
Methods: This was a retrospective monocentric study conducted at a busy district general hospital over a seven-month period. Patient demographic data, operative notes, and radiology reports (by source) were collated for all patients aged ≥16 years presenting with atraumatic abdominal pain who underwent abdominopelvic CT with subsequent surgical intervention (laparoscopy and/or laparotomy).
Results: Seventy-one patients were identified by initial screening, and 10 patients (11 scans) met the criteria for a "major" discrepancy. Overall discrepancy rates were calculated at 5.6% for scans reported off-site compared to 9.9% for reports generated by in-house radiologists.
Conclusion: This study demonstrated lower discrepancy rates in scans reported remotely and can be used as the catalyst for improving aspects of in-house CT reporting.
Keywords: acute abdomen; ct discrepancies; general surgery; in-house reporting; intraoperative findings; laparoscopy; laparotomy; off-site reporting; teleradiology.
Copyright © 2024, Redman et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. NHS Foundation Trust Clinical Governance Department issued approval SUR.EH.22.334. This was a retrospective single-center observational study comparing the hospital’s clinical service outcomes against nationally agreed targets. The study was registered and ethical approval was obtained from the trust’s clinical governance department (SUR.EH.22.334). The requirement for patient consent was waived given the retrospective nature of the study, and formal ethical approval was not required as per the UK National Research Ethics Service guidelines. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures


References
-
- Approach to acute abdominal pain. McNamara R, Dean AJ. Emerg Med Clin North Am. 2011;29:159–173. - PubMed
-
- Mortality in high-risk emergency general surgical admissions. Symons NR, Moorthy K, Almoudaris AM, Bottle A, Aylin P, Vincent CA, Faiz OD. Br J Surg. 2013;100:1318–1325. - PubMed
-
- Multimodality approach for imaging of non-traumatic acute abdominal emergencies. Gangadhar K, Kielar A, Dighe MK, et al. Abdom Radiol (NY) 2016;41:136–148. - PubMed
-
- The Royal College of Surgeons of England. The higher risk general surgical patient: towards improved care for a forgotten group. London (UK): RCSENG - Professional Standards and Regulation; 2011.
LinkOut - more resources
Full Text Sources
Miscellaneous