

Prognostic factors in clear cell sarcoma: an analysis of soft tissue sarcoma in 43 cases
- PMID: 39535601
- PMCID: PMC11560989
- DOI: 10.1007/s00432-024-05980-3
Prognostic factors in clear cell sarcoma: an analysis of soft tissue sarcoma in 43 cases
Abstract
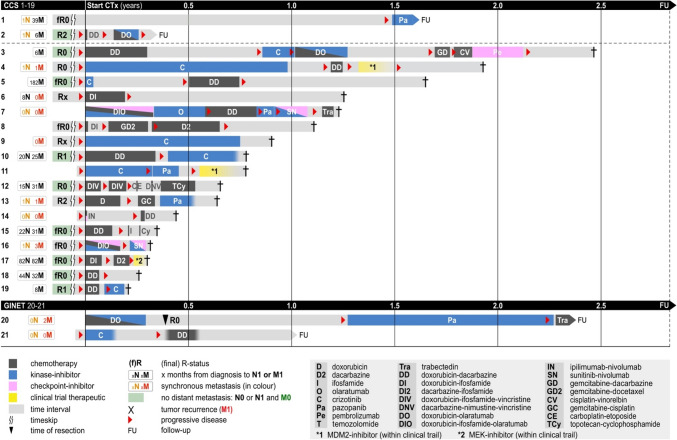
Purpose: Clear cell sarcoma (CCS) of tendons and aponeuroses and CCS-like malignant gastrointestinal neuroectodermal tumor/sarcoma (GINET) are characterized by frequent local and distant relapses, alongside with low efficacy of all systemic treatments. We aimed to collect a comprehensive dataset to identify prognostic factors and treatment outcomes.
Methods: We performed a retrospective single center analysis for diagnosed CCS and GINET on demographic, tumor, treatment and survival data.
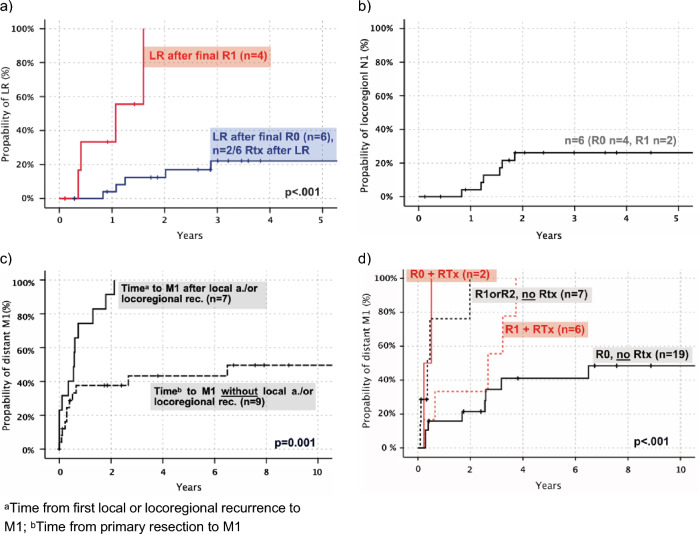
Results: We identified 43 patients (w:25, m:18) with a median follow-up of 35mo and a 5y-OS-rate of 42%. At diagnosis the median age was 42yrs. Median tumor size was 3.6 cm (0.3-11.1 cm), and 24/26 (94%) tissues analyzed at our institute were EWSR1::ATF1-translocation-positive. Distant extremities (incl. knee or elbow) were affected in 72.5%. Of note, 79.5% received an excisional biopsy (benign histology suspected in 30.2%) leading to frequent incomplete resection. Final R0 status correlated significantly (p = 0.017) with longer survival rates compared to R + status in localized CCS (N0M0, 5-yr OS 0% vs 64%). Radiation and systemic treatment had limited antitumor effects while isolated limb perfusion was active in some patients. 18.6% of patients showed lymphatic spread and 20.9% distant metastases. Presence of initial M + was associated with a dismal survival of 1.4 years (M +) vs 7.1 years (M0; p < .001).
Conclusion: We here present one of the largest clinical cohorts of patients with CCS/GINET. Our data underscores the exceptional risk of metastatic disease even in small tumors. As systemic treatment and radiation showed limited efficacy, complete resection was the most important treatment option.
Keywords: CCS; Clear cell sarcoma; EWSR1; Gastrointestinal sarcoma; Malignant melanoma of soft tissue; Prognostic factors.
© 2024. The Author(s).
Conflict of interest statement
Figures

Similar articles
-
Clear cell sarcoma of tendons and aponeuroses: a study of 75 patients.Cancer. 2007 Jan 1;109(1):109-16. doi: 10.1002/cncr.22380. Cancer. 2007. PMID: 17133413
-
Clear cell sarcoma of soft tissue: a clinicopathologic, immunohistochemical, and molecular analysis of 33 cases.Am J Surg Pathol. 2008 Mar;32(3):452-60. doi: 10.1097/PAS.0b013e31814b18fb. Am J Surg Pathol. 2008. PMID: 18300804
-
Clear cell sarcoma of soft tissue: a retrospective review and analysis of 31 cases treated at Istituto Ortopedico Rizzoli.Eur J Surg Oncol. 2014 May;40(5):505-510. doi: 10.1016/j.ejso.2014.01.016. Epub 2014 Feb 2. Eur J Surg Oncol. 2014. PMID: 24560887
-
Clear cell sarcoma of tendons and aponeuroses, and osteoclast-rich tumour of the gastrointestinal tract with features resembling clear cell sarcoma of soft parts: a review and update.J Clin Pathol. 2010 May;63(5):416-23. doi: 10.1136/jcp.2008.057471. J Clin Pathol. 2010. PMID: 20418233 Review.
-
Clear cell sarcoma of tendons and aponeuroses: a historical perspective and tribute to the man behind the entity.Adv Anat Pathol. 2006 Nov;13(6):286-92. doi: 10.1097/01.pap.0000213052.92435.1f. Adv Anat Pathol. 2006. PMID: 17075294 Review.
Cited by
-
[Challenges in the research and diagnosis of rare diseases].Pathologie (Heidelb). 2025 May;46(3):142-151. doi: 10.1007/s00292-025-01426-w. Epub 2025 Apr 3. Pathologie (Heidelb). 2025. PMID: 40178563 German.
-
Clear Cell Sarcoma of Soft Tissues: Radiological Analysis of 14 Patients-MRI Findings Related to Metastatic Disease.Diagnostics (Basel). 2025 Apr 17;15(8):1027. doi: 10.3390/diagnostics15081027. Diagnostics (Basel). 2025. PMID: 40310428 Free PMC article.
References
-
- Al-Refaie WB, Ali MW, Chu DZ et al (2004) Clear cell sarcoma in the era of sentinel lymph node mapping. J Surg Oncol 87(3):126–129. 10.1002/jso.20096 - PubMed
-
- Amin MB, Edge SB, Greene FL et al (eds) (2017) AJCC Cancer Staging Manual, 8th edn. Springer, Switzerland
-
- Behranwala KA, A’Hern R, Omar AM et al (2004) Prognosis of Lymph Node Metastasis in Soft Tissue Sarcoma. Ann Surg Oncol 11:714–719. 10.1245/ASO.2004.04.027 - PubMed
-
- Bianchi G, Charoenlap C, Cocchi S et al (2014) Clear cell sarcoma of soft tissue: a retrospective review and analysis of 31 cases treated at Istituto Ortopedico Rizzoli. Eur J Surg Oncol 40(5):505–510. 10.1016/j.ejso.2014.01.016 - PubMed
-
- Casali PG, Abecassis N, Aro HT et al (2018) Soft tissue and visceral sarcomas: ESMO- EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 29(Suppl 4):51–67 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
