

Switching treatment to cipaglucosidase alfa plus miglustat positively affects patient-reported outcome measures in patients with late-onset Pompe disease
- PMID: 39535661
- PMCID: PMC11561219
- DOI: 10.1186/s41687-024-00805-w
Switching treatment to cipaglucosidase alfa plus miglustat positively affects patient-reported outcome measures in patients with late-onset Pompe disease
Abstract
Background: Late-onset Pompe disease (LOPD), a rare autosomal recessive multisystemic disorder, substantially impacts patients' day-to-day activities, outcomes, and health-related quality of life (HRQoL). The PROPEL trial compared cipaglucosidase alfa plus miglustat (cipa+mig) with alglucosidase alfa plus placebo (alg+pbo) in adult patients with LOPD over 52 weeks and showed improved motor and respiratory function in patients switching treatment from standard-of-care enzyme replacement therapy (ERT) to cipa+mig at baseline. This study evaluated the impact of cipa+mig on patient-reported outcomes (PROs), including HRQoL in ERT-experienced patients, using data from PROPEL.
Methods: PROs evaluated included the Subject's Global Impression of Change (SGIC), Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function Short Form 20a, PROMIS Fatigue Short Form 8a, Rasch-built Pompe-specific Activity (R-PAct), and European Quality of Life-5 Dimensions 5 Response Levels (EQ-5D-5L). The proportions of responders in the cipa+mig arm and the alg+pbo arm were compared via chi-squared or Fisher's exact test (patient-level responder analysis), and least squares (LS) mean differences were calculated for change from baseline at Week 52 of the PRO measures (group-level analysis).
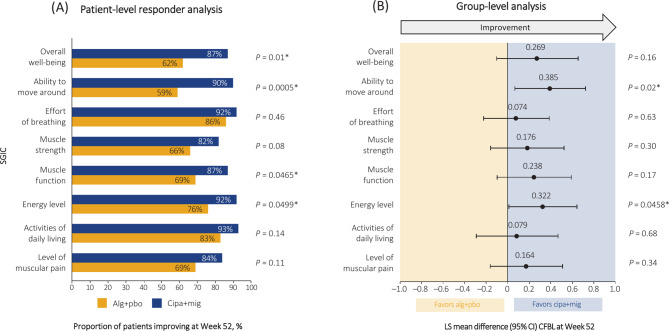
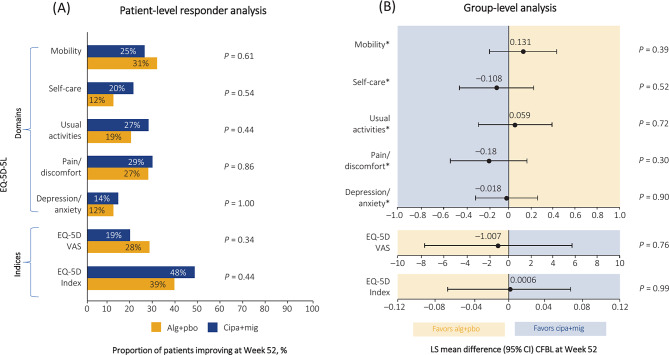
Results: At Week 52, patient-level SGIC responder and group-level SGIC analyses favored cipa+mig compared with alg+pbo across all SGIC domains (e.g. 90 vs. 59% responders in the cipa+mig vs. the alg+pbo group for SGIC ability to move around; P = 0.0005; and LS mean difference 0.385; P = 0.02). Similarly, PROMIS Physical Function and Fatigue domains numerically favored cipa+mig in both analyses (e.g. 50 vs. 40% responders in the cipa+mig vs. alg+pbo arm for PROMIS Physical Function; P = 0.37; and LS mean difference 3.1; P = 0.11). R-PAct for both treatment groups was similar in the patient-level responder analysis, but numerically favored alg+pbo in the group-level analysis (35% responders in both arms; P = 0.95; and LS mean difference -0.8; P = 0.48). Self-care, usual activities, and depression/anxiety domains of EQ-5D-5L numerically favored cipa+mig in both analyses (e.g. 20 vs. 12% responders in the cipa+mig vs. alg+pbo arm for EQ-5D-5L self-care; P = 0.54; and LS mean difference -0.108; P = 0.52).
Conclusions: Overall, switching treatment from alglucosidase alfa to cipa+mig positively impacted PRO measurements during the double-blind period of PROPEL.
Trial registration: NCT03729362; Registration date: November 1, 2018; https://clinicaltrials.gov/study/NCT03729362.
Keywords: Health-related quality of life; Patient-reported Outcome Measurement Information System; Patient-reported outcomes; Pompe disease.
Plain language summary
Late-onset Pompe disease (LOPD) is a rare, multisystemic inherited genetic disease that causes glycogen accumulation in muscles and other body organs, leading to muscle weakness and respiratory insufficiency. LOPD significantly impacts patients’ day-to-day life. Enzyme replacement therapies (ERT) have greatly improved the lives of patients with LOPD. The first approved ERT for LOPD was alglucosidase alfa (alg). To evaluate the effects of a new treatment (cipaglucosidase alfa+miglustat [cipa+mig]) in adult patients with LOPD, two-thirds of patients were switched from alg to cipa+mig and the remaining patients continued receiving alg (alg+placebo [alg+pbo]). We used patient-reported outcome (PRO) questionnaires (asking patients how they feel) to assess changes in patient health. Groups were similar at baseline. Analyses showed that patients improved following cipa+mig treatment for all domains of the PROs Subject’s Global Impression of Change (SGIC; overall physical well-being, effort of breathing, muscle strength, muscle function, ability to move around, activities of daily living, energy level, level of muscular pain) and the Patient-Reported Outcomes Measurement Information System (PROMIS; Physical Function, Fatigue) compared with when treated with alg+pbo. Rasch-built Pompe-specific Activity (R-PAct), a survey evaluating daily activities and social life of patients living with Pompe disease, showed that patients felt similar after cipa+mig and alg+pbo. European Quality of Life-5 Dimensions-5 Response Levels (EQ-5D-5L), a measure of health covering five dimensions, favored cipa+mig in the self-care, usual activities, pain/discomfort and depression/anxiety areas, and alg+pbo for mobility. Overall, changing treatment from alg to cipa+mig positively affects PROs and the patient’s general well-being.
© 2024. The Author(s).
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
