

Retreatment of multiple myeloma with previously refractory drugs
- PMID: 39536293
- PMCID: PMC11700264
- DOI: 10.1182/bloodadvances.2024014723
Retreatment of multiple myeloma with previously refractory drugs
Abstract
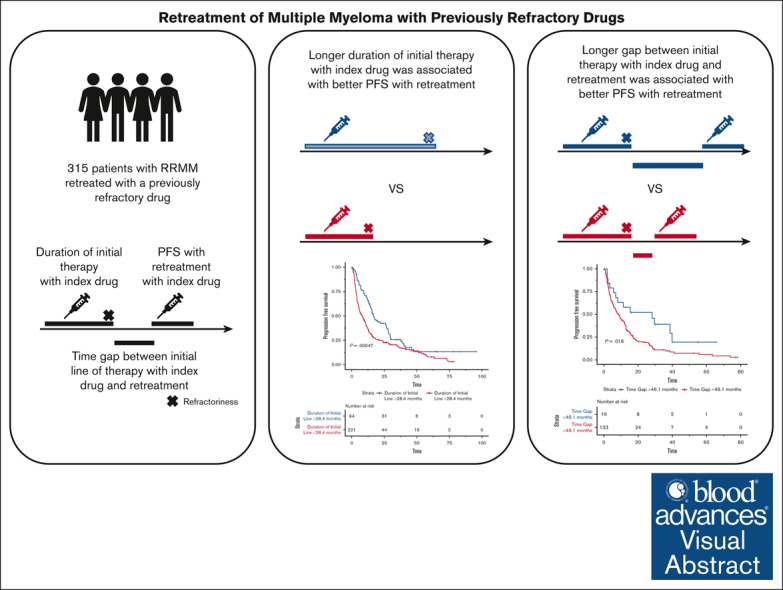
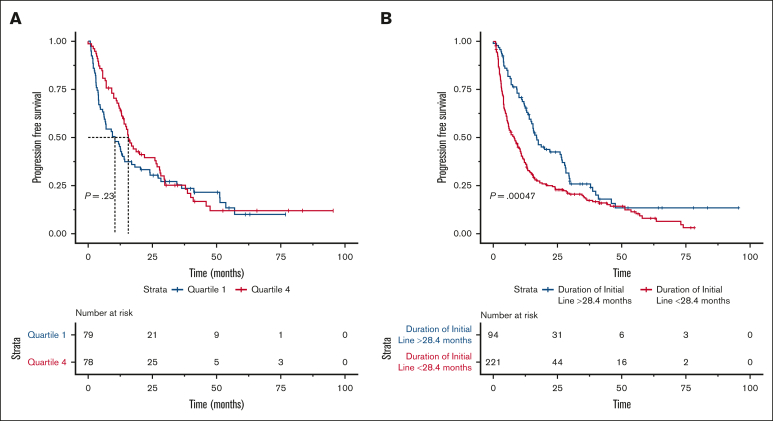
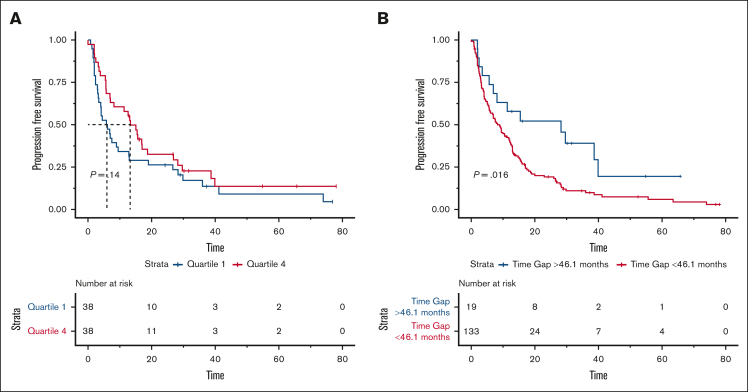
As patients with relapsed/refractory multiple myeloma (RRMM) continue to live longer, they might get exposed to most available drugs and drug classes during the disease course. For such late line RRMM or among patients without access to novel therapies, retreatment with a drug that the disease had previously been refractory to might be one option. In this retrospective study, we describe 315 patients with RRMM at our institution who were retreated with a drug that the disease had been previously refractory to. We found an overall response rate of 56.2% and a median progression-free survival (PFS) of 11 months with retreatment. Patients with a longer time on initial therapy with the index drug (>28.4 months) had a superior PFS with retreatment (median PFS, 16.9 vs 8.1 months; P < .001). Similarly, patients with a longer time gap between the initial line of therapy with index drug and retreatment with index drug (>46.1 months) had better PFS with retreatment (28.2 vs 8.9 months; P = .016). In conclusion, retreatment with a previously refractory drug is a viable therapeutic option for RRMM, with the most significant benefit derived in disease demonstrating sensitivity to initial drug exposure and among those with a longer gap between initial drug exposure and retreatment.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: P.K. reports honoraria from AbbVie (institution), AstraZeneca, BeiGene, MustangBio, Pharmacyclics, and Sanofi (institution); consulting or advisory role with Sanofi (institution); research funding from AbbVie (institution), Amgen (institution), Bristol Myers Squibb/Celgene (institution), GlaxoSmithKline (institution), Ichnos Sciences (institution), Karyopharm Therapeutics (institution), Regeneron (institution), Sanofi (institution), Sorrento Therapeutics (institution), and Takeda (institution); and travel, accommodations, and expenses from GlaxoSmithKline, Janssen, and Sanofi. A.D. reports consulting or advisory role with Janssen Research & Development; research funding from Alnylam (institution), Celgene (institution), Janssen Oncology (institution), Pfizer (institution), Prothena, and Takeda (institution); and travel, accommodations, and expenses from Janssen Oncology, Pfizer, and Prothena. D.D. reports consulting or advisory roles with Alexion Pharmaceuticals, Apellis Pharmaceuticals, Bristol Myers Squibb, J&J Innovative Medicine, Legend Biotech, Novartis, and Sanofi; and research funding from K36 Therapeutics (institution). M.A.G. reports honoraria from AbbVie, Akcea Therapeutics, Alnylam, Amgen, Apellis Pharmaceuticals, Celgene, Janssen Oncology, Juno/Celgene, Med Learning Group, Prothena, Research to Practice, Sanofi, and Telix Pharmaceuticals; consulting or advisory roles with Bristol Myers Squibb/Sanofi and Prothena; and travel, accommodations, and expenses from Celgene, Novartis, and Prothena. W.I.G. reports consulting or advisory role with Amgen (institution); research funding from Bristol Myers Squibb Foundation (institution) and ORIC Pharmaceuticals (institution); and patents, royalties, and other intellectual property (patent number 10996224 for assessing and treating precursor plasma cell disorders). N.L. reports stock and other ownership interests with AbbVie, Senseonics, and Verrica Pharmaceuticals; and research funding from Omeros. Y.L. reports consulting or advisory roles with Adicet Bio (institution), Bristol Myers Squibb (institution), Caribou Biosciences (institution), Chimeric Therapeutics (institution), Fosun Kite (institution), Genentech (institution), Janssen Oncology (institution), Kite/Gilead (institution), Nektar (institution), NexImmune (institution), Pfizer (institution), Regeneron (institution), Sanofi (institution), and Vineti (institution); and research funding from Bristol Myers Squibb (institution) and Janssen Oncology (institution). S.K.K. reports consulting or advisory roles with AbbVie (institution), Bristol Myers Squibb/Celgene (institution), Genentech/Roche (institution), Janssen Oncology (institution), K36 (institution), Pfizer (institution), Regeneron (institution), Sanofi (institution), and Takeda (institution); research funding from AbbVie (institution), Allogene Therapeutics (institution), Bristol Myers Squibb/Celgene (institution), CARsgen Therapeutics (institution), GlaxoSmithKline (institution), Janssen Oncology (institution), MedImmune (institution), Novartis (institution), Regeneron (institution), Roche/Genentech (institution), Sanofi (institution), and Takeda (institution); and travel, accommodations, and expenses from AbbVie and Pfizer. The remaining authors declare no competing financial interests.
Figures
References
-
- Binder M, Nandakumar B, Rajkumar SV, et al. Mortality trends in multiple myeloma after the introduction of novel therapies in the United States. Leukemia. 2022;36(3):801–808. - PubMed
-
- Kumar SK. Recycling therapies for myeloma: the need for prospective trials. Cancer. 2019;125(17):2920–2922. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
