

Safety of inpatient care in surgical settings: cohort study
- PMID: 39537329
- PMCID: PMC11558683
- DOI: 10.1136/bmj-2024-080480
Safety of inpatient care in surgical settings: cohort study
Abstract
Objectives: To estimate the frequency, severity, and preventability of adverse events associated with perioperative care, and to describe the setting and professions concerned.
Design: Multicenter retrospective cohort study.
Setting: 11 US hospitals.
Participants: 1009 patients from a randomly selected sample of 64 121 adults admitted for surgery during 2018.
Main outcome measures: Adverse events during inpatient perioperative care were assessed using a trigger method, identifying information previously associated with similar events, and from a comprehensive review of electronic health records. Trained nurses reviewed all records and flagged admissions with possible adverse events, which were then adjudicated by physicians, who confirmed the occurrence and characteristics of the events. Adverse events were classified as major if they resulted in serious harm requiring substantial intervention or prolonged recovery, involved a life threatening event, or led to a fatal outcome. Potentially preventable events included those definitively, probably, or possibly preventable.
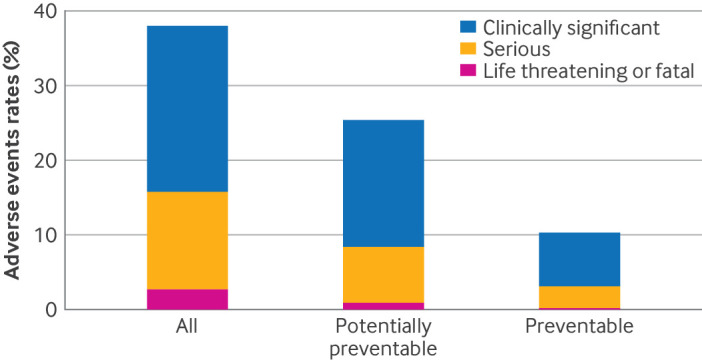
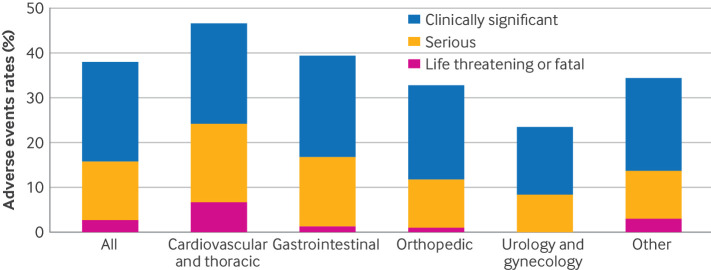
Results: Among 1009 patients reviewed, adverse events were identified in 38.0% (95% confidence interval 32.6 to 43.4), with major adverse events occurring in 15.9% (12.7 to 19.0). Of 593 identified adverse events, 353 (59.5%) were potentially preventable and 123 (20.7%) were definitely or probably preventable. The most common adverse events were related to surgical procedures (n=292, 49.3%), followed by adverse drug events (n=158, 26.6%), healthcare associated infections (n=74, 12.4%), patient care events (n=66, 11.2%), and blood transfusion reactions (n=3, 0.5%). Adverse events were most frequent in general care units (n=289, 48.8%), followed by operating rooms (n=155, 26.1%), intensive care units (n=77, 13.0%), recovery rooms (n=20, 3.3%), emergency departments (n=11, 1.8%), and other in-hospital locations (n=42, 7.0%). Professions most involved were attending physicians (n=531, 89.5%), followed by nurses (n=349, 58.9%), residents (n=294, 49.5%), advanced level practitioners (n=169, 28.5%), and fellows (n=68, 11.5%).
Conclusions: Adverse events were identified in more than one third of patients admitted to hospital for surgery, with nearly half of the events classified as major and most potentially preventable. These findings emphasize the critical need for ongoing improvement in patient safety, involving all health professionals, throughout perioperative care.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from Controlled Risk Insurance Company and the Risk Management Foundation of the Harvard Medical Institutions for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Kohn LT, Corrigan JM, Donaldson MS, eds. To err is human: building a safer health system. National Academies Press, 2000. - PubMed
-
- Richards MK, McAteer JP, Drake FT, Goldin AB, Khandelwal S, Gow KW. A national review of the frequency of minimally invasive surgery among general surgery residents: assessment of ACGME case logs during 2 decades of general surgery resident training. JAMA Surg 2015;150:169-72. 10.1001/jamasurg.2014.1791 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical