

The Extent of Tumor in the Peritoneum and Liver Influences Outcomes After Surgery for Synchronous Liver and Peritoneal Colorectal Metastases: A Cohort Study
- PMID: 39537942
- PMCID: PMC11561098
- DOI: 10.1007/s12029-024-01139-y
The Extent of Tumor in the Peritoneum and Liver Influences Outcomes After Surgery for Synchronous Liver and Peritoneal Colorectal Metastases: A Cohort Study
Abstract
Purpose: Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRSH) or liver resection have led to increased survival in patients with peritoneal or liver metastases of colorectal cancer. Selected patients undergo concomitant CRSH and liver resection. Differences in survival and morbidity between patients who underwent concomitant surgery, CRSH or liver resection for peritoneal and/or liver metastases were compared.
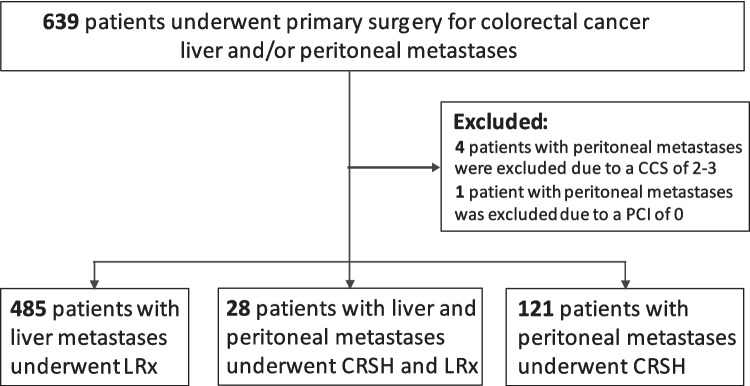
Methods: Patients who underwent liver resection and/or CRSH for colorectal liver and/or peritoneal metastases, 2006-2016, were included. Regression analysis was used to evaluate the associations between baseline characteristics and survival.
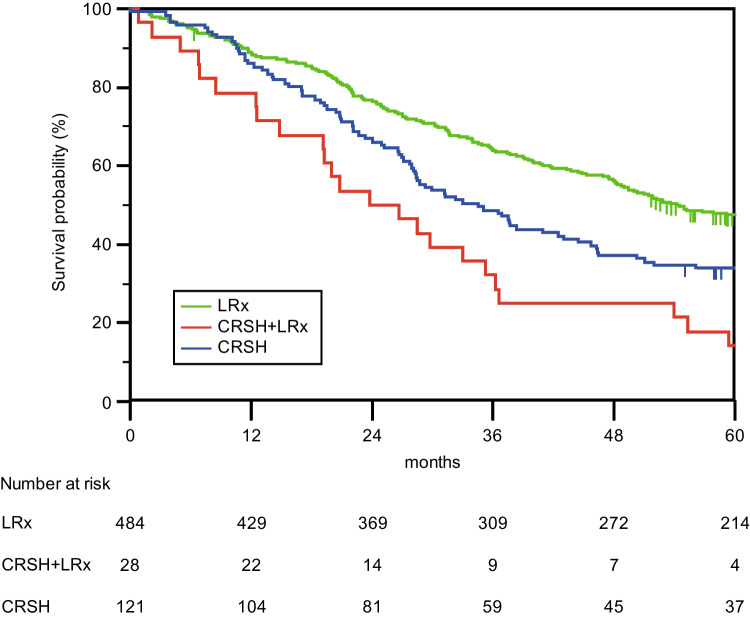
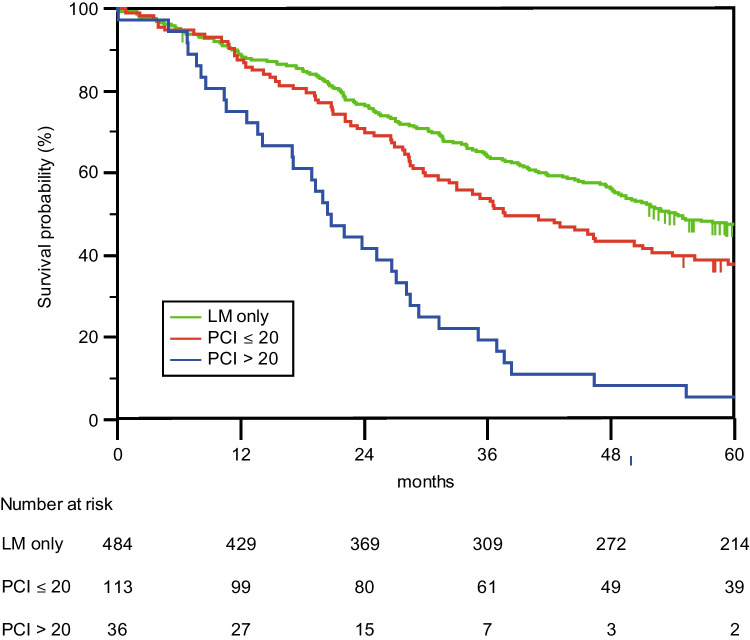
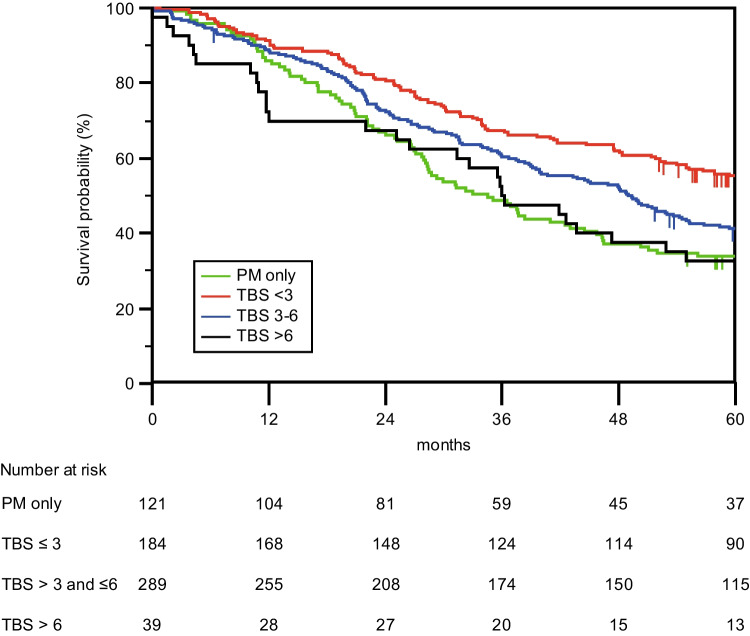
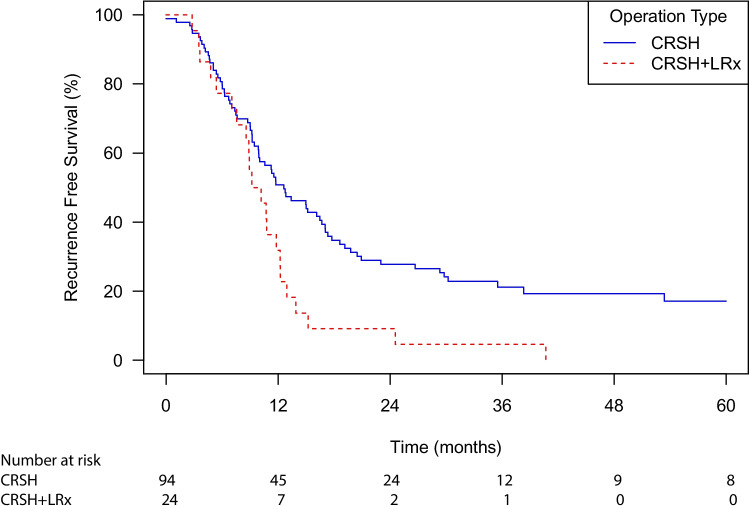
Results: Overall, 634 patients were studied. Twenty-eight patients had peritoneal and liver metastases, 121 patients had peritoneal metastases only, and 485 patients had isolated liver metastases. Median survival after concomitant treatment was 23.8 months (95% CI 12.8-43.8), after CRSH 34.5 months (95% CI 27.1-41.9), and after liver resection 54.2 months (95% CI 47.4-61.0) (p < 0.001). Increased hepatic tumor burden (HR 3.2, 95% CI 1.8-5.8) and high-volume peritoneal disease (HR 6.0, 95% CI 3.7-9.8) were associated with decreased survival in multivariate analysis. Postoperative complications according to a Clavien-Dindo score > 3a were observed in 11% in the liver resection group, 15% in the CRSH group, and 11% in the concomitant treatment group (p = 0.945).
Conclusions: Patients treated with concomitant surgery for liver and peritoneal metastases experienced a shorter median overall survival than patients treated for metastases at an isolated site but had a similar rate of severe postoperative complications. The extent of peritoneal spread seemed to impact survival more than the tumor burden in the liver.
Keywords: CRS; Colorectal cancer; HIPEC; Liver metastases; Liver resection; Peritoneal metastases.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Sugarbaker PH. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in the management of gastrointestinal cancers with peritoneal metastases: progress toward a new standard of care. Cancer Treat Rev. 2016;48:42–9. - PubMed
-
- Baratti D, Kusamura S, Pietrantonio F, et al. Progress in treatments for colorectal cancer peritoneal metastases during the years 2010–2015. A systematic review. Crit Rev Oncol Hematol. 2016;100:209–22. - PubMed
-
- Franko J, Shi Q, Meyers JP, et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomized trials from the analysis and research in cancers of the digestive system (ARCAD) database. Lancet Oncol. 2016;17(12):1709–19. - PubMed
-
- van der Geest LG, Lam-Boer J, Koopman M, et al. Nationwide trends in incidence, treatment and survival of colorectal cancer patients with synchronous metastases. Clin Exp Metastasis. 2015;32(5):457–65. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical