

Cost analysis of adding hypertension and diabetes management into routine HIV care in Mbarara and Ibanda districts, Uganda
- PMID: 39538306
- PMCID: PMC11559216
- DOI: 10.1186/s12913-024-11825-z
Cost analysis of adding hypertension and diabetes management into routine HIV care in Mbarara and Ibanda districts, Uganda
Abstract
Background: In 2016, Uganda introduced services for hypertension and diabetes in selected HIV clinics. We evaluated the costs associated with scaling up these services in HIV clinics in Mbarara and Ibanda districts, Uganda.
Methods: We estimated the annual costs of providing hypertension and diabetes services using an activity-based costing approach from the health system perspective in ten randomly selected HIV clinics in Mbarara and Ibanda districts. Cost inputs included 2023 data on costs of medications, health provider time, salaries, training costs, and monitoring costs. We determined the average annual cost and medication costs for hypertension and diabetes treatment per enrolled adult patient, stratified by type of health facility.
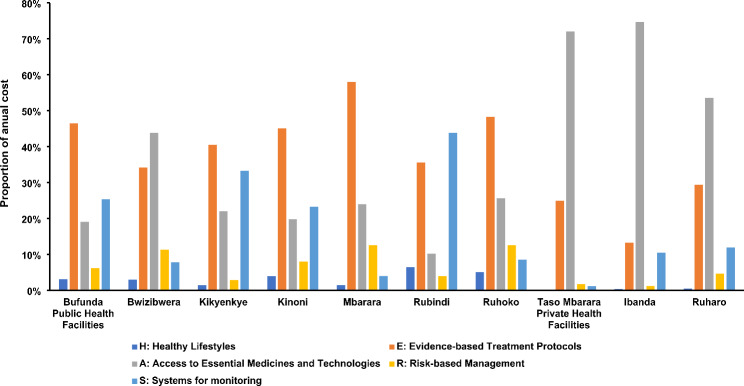
Results: The total annual cost of hypertension and diabetes management services in ten selected HIV clinics was estimated to be $413,850 (range: $8,386 - 186,973). The annual average clinic-level cost per enrolled patient was estimated at $14 (range: $7 - 31). Of the total annual cost, the cost of provider time for initial and follow-up visits represented the largest cost component in 5/10 clinics (mean: 37%, range [13-58%]). In 4/10 clinics, the major cost components were the costs of medication, diagnostic tests, and related supplies (mean: 37%, range [10-75%]). The average cost per enrolled adult patient was $11 at public facilities and $21 in private not-for-profit facilities. The average medication cost per patient for hypertension was $24 (range: $7 - 97) annually; $13 at public facilities and $50 at private not-for-profit facilities. For diabetes treatment, the average annual medication cost per patient was estimated at $14 (range: $6 - 35); $11 at public facilities and $22 at private not-for-profit facilities.
Conclusion: Adding hypertension and diabetes management to routine HIV care might be feasible based on the estimated annual cost per patient. Hypertension and diabetes treatment was more costly in private not-for-profit facility-based clinics than at public facilities. This variation was primarily driven by higher medication procurement prices at private facilities, revealing a potential area for optimizing costs through improved procurement practices.
Keywords: Cost analysis; Diabetes; HIV; Hypertension; Uganda.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Duffy M, Ojikutu B, Andrian S, Sohng E, Minior T, Hirschhorn LR. <ArticleTitle Language=“En”>Non-communicable diseases and HIV care and treatment: models of integrated service delivery. Tropical Med Int Health. 2017;22(8):926–37. - PubMed
-
- Haldane V, Legido-Quigley H, Chuah FLH, Sigfrid L, Murphy G, Ong SE, et al. Integrating cardiovascular diseases, hypertension, and diabetes with HIV services: a systematic review. AIDS Care. 2018;30(1):103–15. - PubMed
-
- Monroe AK, Glesby MJ, Brown TT. Diagnosing and managing diabetes in HIV-infected patients: current concepts. Clin Infect Dis. 2015;60(3):453–62. - PubMed
-
- Sarkar S, Brown TT. Diabetes in people living with HIV. Endotext. 2019.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
