

Unraveling Facial Nerve Palsy: A Case Series Highlighting Diagnostic and Therapeutic Challenges
- PMID: 39539892
- PMCID: PMC11559602
- DOI: 10.7759/cureus.71445
Unraveling Facial Nerve Palsy: A Case Series Highlighting Diagnostic and Therapeutic Challenges
Abstract
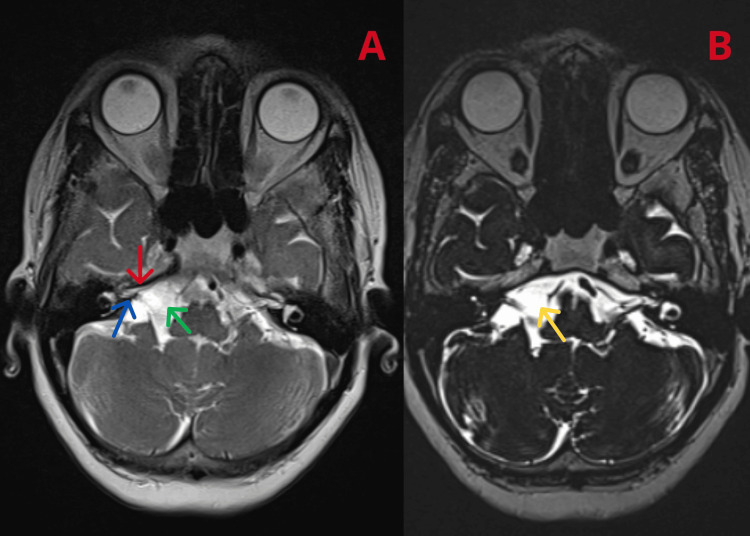
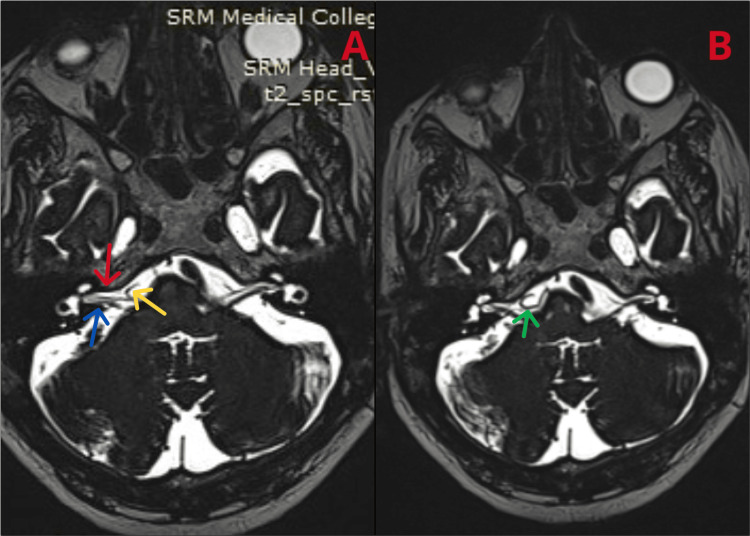
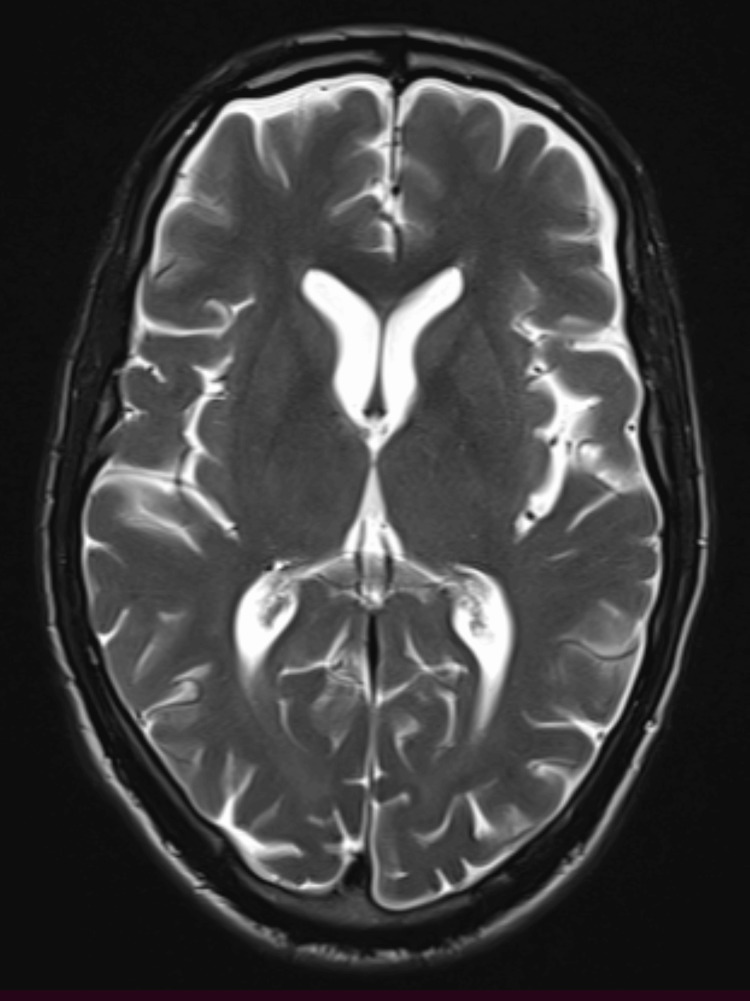
Facial nerve palsy (FNP) may arise from multiple etiological reasons, including anatomical anomalies, circulatory complications, and infectious agents. This case series underscores the importance of a comprehensive diagnostic approach to identify the precise etiology, including structural abnormalities, vascular anomalies, or infectious illnesses. Here, we present three distinct occurrences of FNP, emphasizing the varied diagnostic difficulties and therapeutic strategies. It includes an arachnoid cyst, which when occurring at the cerebellopontine angle can affect multiple cranial nerves, specifically the seventh and eighth cranial nerve, a neurovascular compression syndrome, where the anterior inferior cerebellar artery loops around the facial nerve. Most often, this scenario causes hemifacial spasms, which in our scenario manifests as FNP. Lyme disease is a tick-borne disease that affects multiple cranial nerves, specifically the facial nerve. Effective management necessitates a focused treatment strategy that tackles the symptoms and the underlying disease. Advanced imaging techniques, serological tests, and a tailored treatment approach are essential for effective diagnosis, can have significant implications for patient well-being, and necessitate a thorough evaluation to identify underlying causes. This case series illustrates the diverse etiologies of FNP, emphasizing the need for comprehensive diagnostic strategies and targeted treatments. As clinicians encounter FNPs more often, this case series can help physicians understand facial palsy better. Continuous research and clinical awareness are vital for improving patient outcomes in cases of FNP.
Keywords: arachnoid cyst; lyme disease; seventh cranial nerve palsy; unilateral facial nerve palsy; vascular loop compression.
Copyright © 2024, T et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Facial nerve compression by the posterior inferior cerebellar artery causing facial pain and swelling: a case report.J Med Case Rep. 2014 Mar 25;8:105. doi: 10.1186/1752-1947-8-105. J Med Case Rep. 2014. PMID: 24661509 Free PMC article.
-
Facial nerve palsy may indicate coronary artery lesions in Kawasaki disease.Clin Rheumatol. 2021 Oct;40(10):4191-4197. doi: 10.1007/s10067-021-05791-8. Epub 2021 May 31. Clin Rheumatol. 2021. PMID: 34059986
-
Arachnoid cyst of the cerebellopontine angle associated with gliosis of the eighth cranial nerve.J Clin Neurosci. 2007 Jul;14(7):700-2. doi: 10.1016/j.jocn.2006.01.013. Epub 2007 May 1. J Clin Neurosci. 2007. PMID: 17475499
-
Acute onset of facial nerve palsy associated with Lyme disease in a 6 year-old child.Pediatr Dent. 2002 Nov-Dec;24(6):572-4. Pediatr Dent. 2002. PMID: 12528951 Review.
-
The many faces of hemifacial spasm: differential diagnosis of unilateral facial spasms.Mov Disord. 2011 Aug 1;26(9):1582-92. doi: 10.1002/mds.23692. Epub 2011 Apr 5. Mov Disord. 2011. PMID: 21469208 Review.
References
-
- [The epidemiology of Bell's palsy] De Diego-Sastre JI, Prim-Espada MP, Fernández-García F. Rev Neurol. 2005;41:287–290. - PubMed
-
- Bell's palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Peitersen E. Acta Otolaryngol Suppl. 2002:4–30. - PubMed
-
- Bilateral facial paralysis: case presentation and discussion of differential diagnosis. Jain V, Deshmukh A, Gollomp S. https://link.springer.com/article/10.1111/j.1525-1497.2006.00466.x J Gen Intern Med. 2006;21:0–10. - PMC - PubMed
-
- Prevalence and natural history of arachnoid cysts in adults. Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. J Neurosurg. 2013;118:222–231. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials