

Double Iatrogenic Esophageal and Duodenal Injury Induced by Endoscopic Retrograde Cholangiopancreatography: A Case Report
- PMID: 39539914
- PMCID: PMC11558017
- DOI: 10.7759/cureus.71355
Double Iatrogenic Esophageal and Duodenal Injury Induced by Endoscopic Retrograde Cholangiopancreatography: A Case Report
Abstract
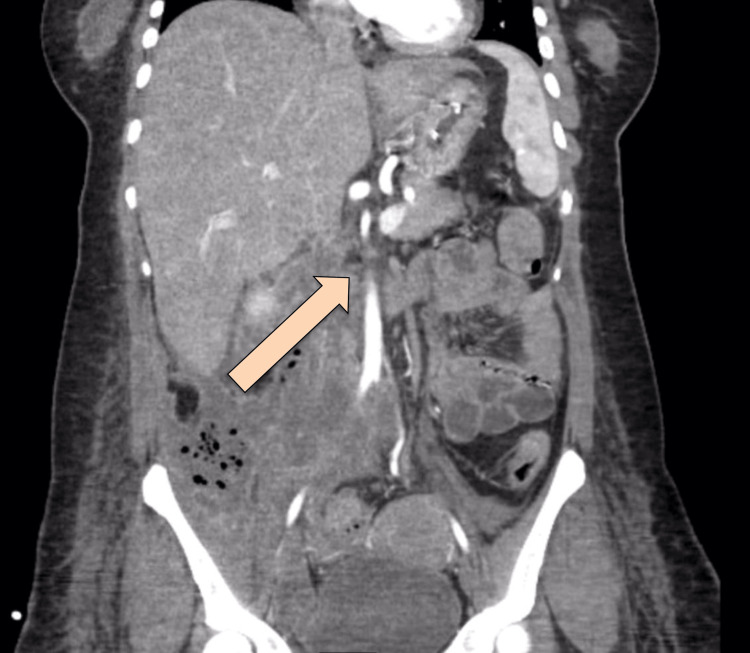
Endoscopic retrograde cholangiopancreatography (ERCP) is a frequently performed procedure in the management of hepatobiliary diseases that can be conducted as a therapeutic or diagnostic procedure. Also, it can be done with or without sphincterotomy and stent insertion. Hemorrhage is one of the most common post-ERCP complications, which can be presented as late as 10 days. Other complications include post-ERCP pancreatitis and perforation. Gut perforation during ERCP is rare but often lethal. Here we present a 35-year-old female who was admitted to the hospital through the ER as a case of obstructive jaundice with common bile duct (CBD) stone. ERCP with stent insertion was performed for the patient to relieve the obstruction; however, intra-procedural retroperitoneal perforation was encountered.
Keywords: duodenal injury; endoscopic retrograde cholangiopancreatography; endoscopy; esophageal injury; iatrogenic.
Copyright © 2024, Albugami et al.
Conflict of interest statement
Human subjects: Consent was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures







References
-
- Classification and management of perforations complicating endoscopic sphincterotomy. Howard TJ, Tan T, Lehman GA, et al. Surgery. 1999;126:658–665. - PubMed
-
- ERCP-related perforations: risk factors and management. Enns R, Eloubeidi MA, Mergener K, Jowell PS, Branch MS, Pappas TM, Baillie J. Endoscopy. 2002;34:293–298. - PubMed
-
- Validity of clinical criteria in the management of endoscopic retrograde cholangiopancreatography related duodenal perforations. Assalia A, Suissa A, Ilivitzki A, et al. Arch Surg. 2007;142:1059–1064. - PubMed
Publication types
LinkOut - more resources
Full Text Sources