

The proinflammatory status, based on preoperative interleukin-6, predicts postpancreatectomy acute pancreatitis and associated postoperative pancreatic fistula after pancreaticoduodenectomy
- PMID: 39540557
- PMCID: PMC11771581
- DOI: 10.1111/jgh.16797
The proinflammatory status, based on preoperative interleukin-6, predicts postpancreatectomy acute pancreatitis and associated postoperative pancreatic fistula after pancreaticoduodenectomy
Abstract
Background and aim: Early predictors of morbidity after pancreaticoduodenectomy (PD) can guide tailored postoperative management. Preoperative inflammatory data in patients who underwent PD remained poorly studied in investigating the clinical significance of predicting postpancreatectomy acute pancreatitis (PPAP) and PPAP-associated postoperative pancreatic fistula (POPF).
Methods: The clinical data of 467 patients receiving PD between January 2020 and December 2022 were retrospectively reviewed. Preoperative inflammatory data were stratified according to PPAP, and independent risk factors were analyzed. Multivariate logistic regression and subgroup analyses were conducted to compare risk factors of PPAP-associated POPF and non-PPAP-associated POPF.
Results: PPAP occurred in 17.6% of patients. The incidence of other complications increased following PPAP. Among the preoperative inflammatory factors, only interleukin-6 (IL-6) increased (P < 0.001), leading to a higher incidence of PPAP and POPF (P < 0.001; P = 0.002). The area under the curve of IL-6 in predicting PPAP was 0.71 (0.65-0.77; P < 0.001). Abnormal preoperative IL-6 levels (odds ratio [OR]: 5.01; P < 0.001), soft pancreatic texture (OR: 2.15; P = 0.007), and pathology (OR: 2.03; P = 0.012) were independent risk factors for PPAP. The subgroup analysis showed that increased IL-6 (OR: 1.01; P = 0.006) and soft pancreatic texture (OR: 2.05; P = 0.033) resulted in a higher risk of PPAP-associated POPF, while increased IL-8 (OR: 1.01; P = 0.007), older age (OR: 1.05; P = 0.008), and higher body mass index (OR: 1.12; P = 0.021) correlated with non-PPAP-associated POPF.
Conclusion: PPAP is common after PD; a high preoperative IL-6 level can predict its occurrence, in addition to associated POPF, which could be due to a preoperative proinflammatory status.
Keywords: PPAP‐associated postoperative pancreatic fistula; interleukin‐6; pancreaticoduodenectomy; postpancreatectomy acute pancreatitis; proinflammatory status.
© 2024 The Author(s). Journal of Gastroenterology and Hepatology published by Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Figures
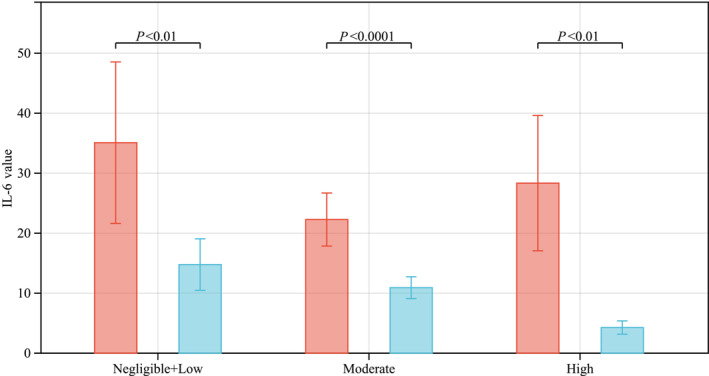
 , PPAP;
, PPAP;  , No PPAP.
, No PPAP.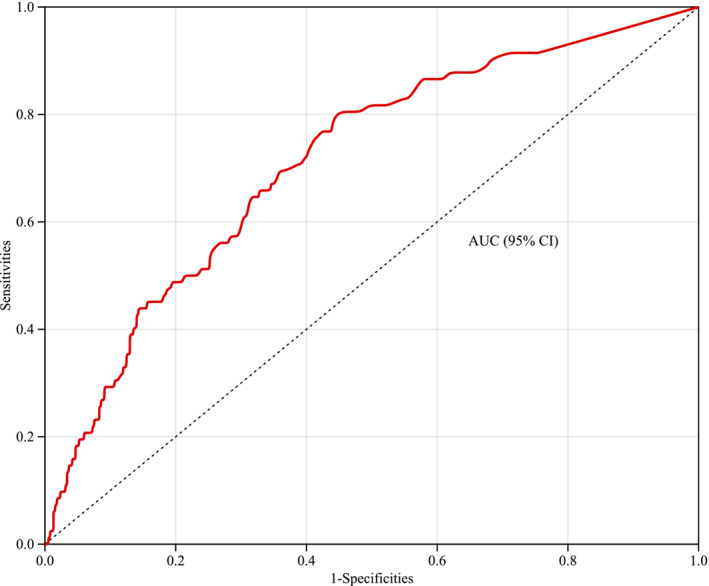
 , 0.71 (0.77–0.65).
, 0.71 (0.77–0.65).Similar articles
-
Postpancreatectomy acute pancreatitis in pancreaticoduodenectomy and distal pancreatectomy: a retrospective cohort study on risk factors and clinical outcomes.Surg Endosc. 2025 Jul;39(7):4225-4234. doi: 10.1007/s00464-025-11787-1. Epub 2025 May 19. Surg Endosc. 2025. PMID: 40389656
-
Enhancement pattern of the pancreatic parenchyma predicts postpancreatectomy acute pancreatitis after pancreaticoduodenectomy.Eur Radiol. 2024 Jan;34(1):6-15. doi: 10.1007/s00330-023-09927-z. Epub 2023 Jul 28. Eur Radiol. 2024. PMID: 37505246
-
Machine learning model-based prediction of postpancreatectomy acute pancreatitis following pancreaticoduodenectomy: A retrospective cohort study.World J Gastroenterol. 2025 Feb 28;31(8):102071. doi: 10.3748/wjg.v31.i8.102071. World J Gastroenterol. 2025. PMID: 40062328 Free PMC article.
-
Prediction of postoperative pancreatic fistula and pancreatitis after pancreatoduodenectomy or distal pancreatectomy: A review.Scand J Surg. 2023 Jun;112(2):126-134. doi: 10.1177/14574969231167781. Epub 2023 Apr 21. Scand J Surg. 2023. PMID: 37083016 Review.
-
Postoperative pancreatitis and pancreatic fistulae: a review of current evidence.HPB (Oxford). 2023 Sep;25(9):1011-1021. doi: 10.1016/j.hpb.2023.05.007. Epub 2023 May 11. HPB (Oxford). 2023. PMID: 37301633 Review.
References
-
- Bannone E, Andrianello S, Marchegiani G, Masini G, Malleo G, Bassi C, Salvia R. Postoperative acute pancreatitis following pancreaticoduodenectomy: a determinant of fistula potentially driven by the intraoperative fluid management. Ann. Surg. 2018; 268: 815–822. - PubMed
-
- Marchegiani G, Barreto SG, Bannone E et al. Postpancreatectomy acute pancreatitis (PPAP): definition and grading from the International Study Group for Pancreatic Surgery (ISGPS). Ann. Surg. 2022; 275: 663–672. - PubMed
-
- Chen H, Wang C, Shen Z et al. Postpancreatectomy acute pancreatitis after pancreaticoduodenectomy: a distinct clinical entity. Ann. Surg. 2023; 278: e278–e283. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
