

Cost-Effectiveness of Computer-Assisted Cognitive Behavioral Therapy for Depression Among Adults in Primary Care
- PMID: 39541120
- PMCID: PMC11565263
- DOI: 10.1001/jamanetworkopen.2024.44599
Cost-Effectiveness of Computer-Assisted Cognitive Behavioral Therapy for Depression Among Adults in Primary Care
Abstract
Importance: Approximately 1 in 5 adults are diagnosed with depression in their lifetime. However, less than half receive help from a health professional, with the treatment gap being worse for individuals with socioeconomic disadvantage. Computer-assisted cognitive behavioral therapy (CCBT) is an effective and convenient strategy to treat depression; however, its cost-effectiveness in a sociodemographically diverse population remains unknown.
Objective: To evaluate the cost-effectiveness of clinician-supported CCBT compared with treatment as usual (TAU) in a primary care population with a substantial number of patients with low income, limited computer or internet access, and lack of college education.
Design, setting, and participants: This economic evaluation was a randomized clinical trial-based cost-effectiveness analysis. The trial was conducted at the Departments of Family and Geriatric Medicine and Internal Medicine at the University of Louisville. Enrollment occurred from June 24, 2016, to May 13, 2019. Participants had mild to moderate depression and were followed up for 6 months after treatment completion. The last follow-up assessment was conducted on January 30, 2020. Statistical analysis was performed from August 2023 to August 2024.
Exposure: CCBT intervention was provided for 12 weeks and included 9 modules ranging from behavioral activation and cognitive restructuring to relapse prevention strategies, supported by telephonic sessions with a clinician, in addition to TAU, which included standard clinical management in primary care.
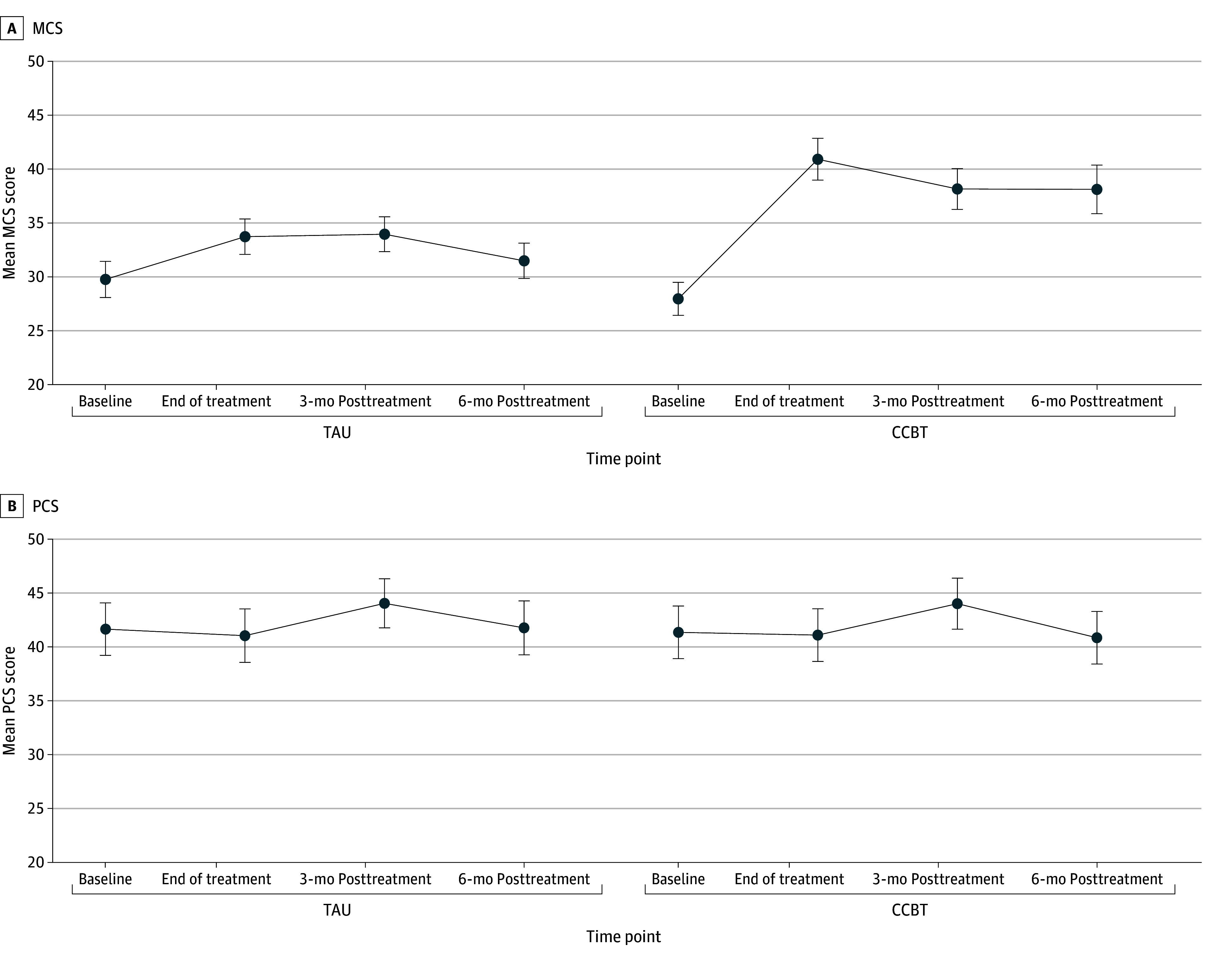
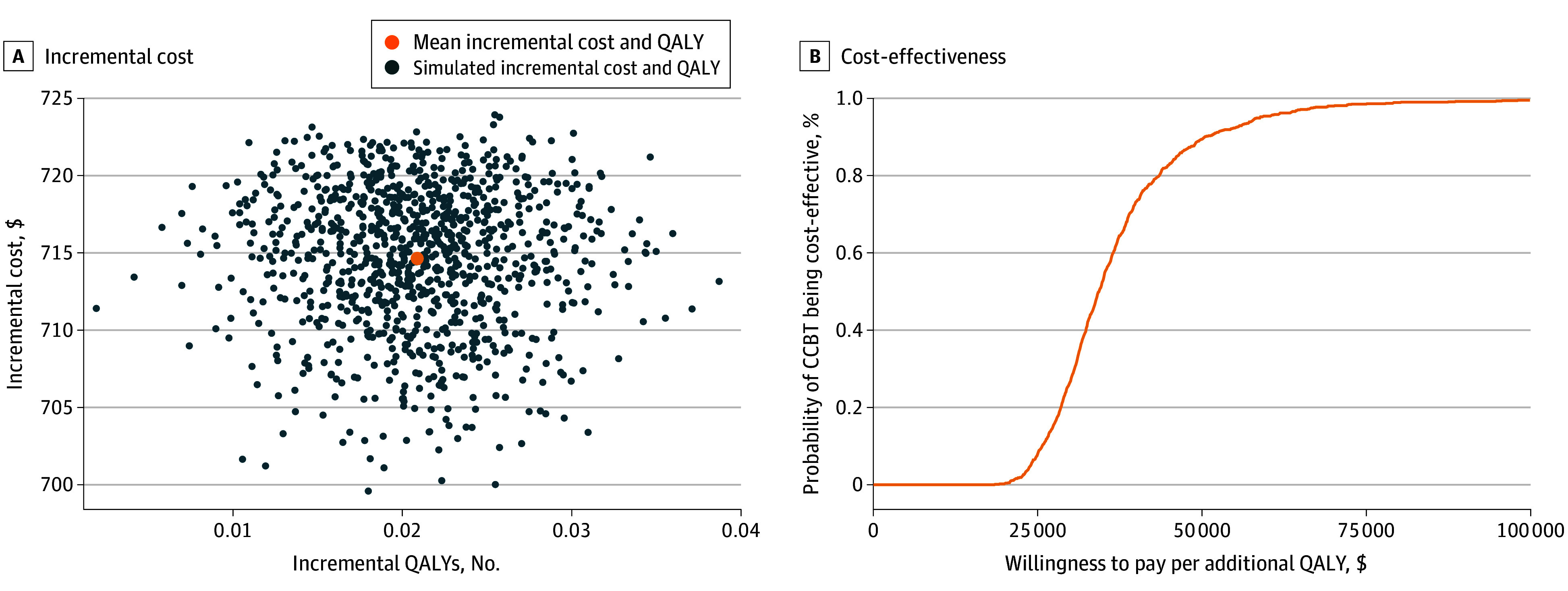
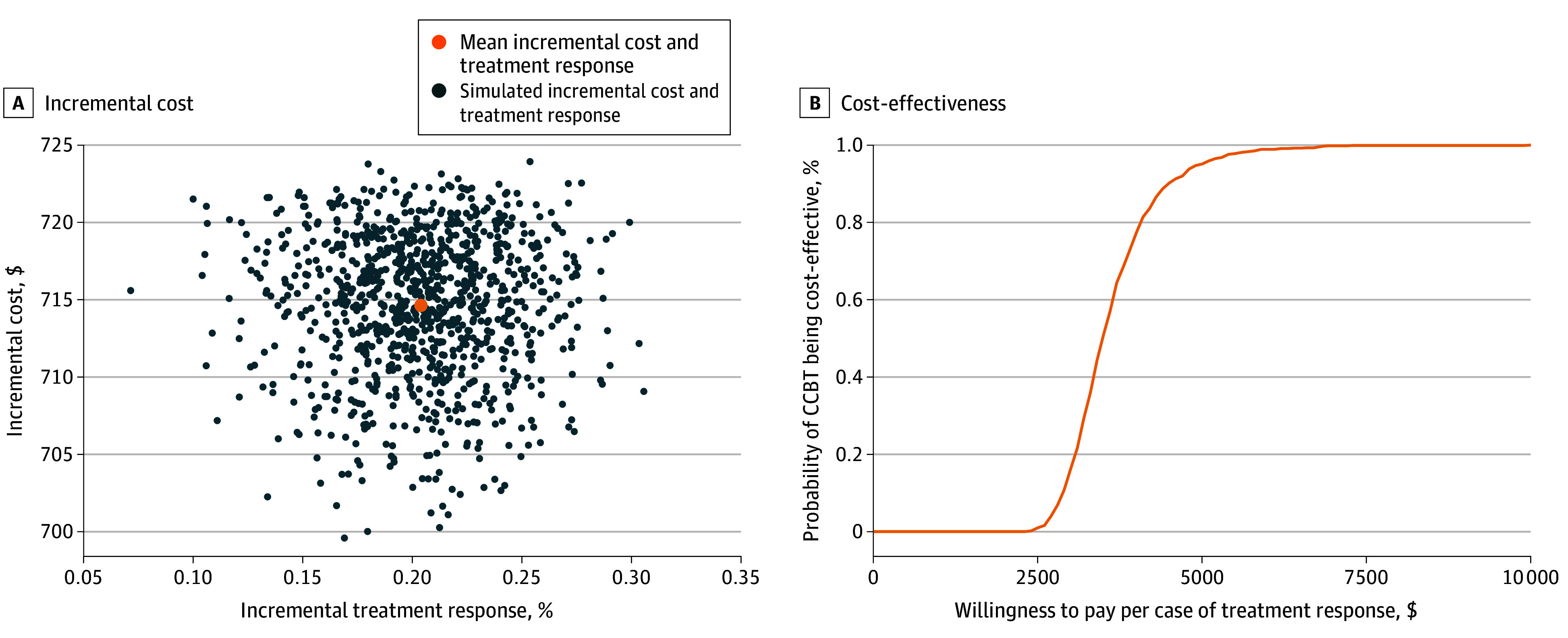
Main outcomes and measures: The primary health outcome was quality-adjusted life years (QALYs), estimated using the Short-Form 12 questionnaire (SF-12). The secondary outcome was treatment response, defined as at least 50% improvement in the Patient Health Questionnaire. The intervention cost included sessions with mental health clinicians and the cost of the CCBT software, plus the cost of loaner computer and internet data plan for low-resource households. An incremental cost-effectiveness ratio (ICER) was computed, while adjusting for baseline scores, age, and sex. The cost-effectiveness acceptability curve presented the probability of CCBT being cost-effective for a range of willingness-to-pay values.
Results: Among the 175 primary care patients included in this study, 148 (84.5%) were female; 48 (27.4%) were African American, 2 (1.2%) were American Indian or Alaska Native, 4 (2.5%) were Hispanic, 106 (60.5%) were White, and 15 (8.6%) were multiracial; and the mean (SD) age was 47.03 (13.15) years. CCBT was associated with better quality of life and higher chance of treatment response at the posttreatment and 6-month time points, compared with the TAU group. The ICER for CCBT was $37 295 (95% CI, $22 724-$66 546) per QALY, with a probability of 89.4% of being cost-effective at a willingness-to-pay threshold of $50 000/QALY. The ICER per case of treatment response was $3623 (95% CI, $2617-$5377).
Conclusions and relevance: In this trial-based economic evaluation, CCBT was found to be cost-effective, compared with TAU, in primary care patients with depression. As this study included individuals with low income and with limited internet access who are underrepresented in cost-effectiveness studies, it has important policy implications for addressing unmet needs in sociodemographically diverse populations.
Conflict of interest statement
Figures
Similar articles
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.Health Technol Assess. 2006 Sep;10(33):iii, xi-xiv, 1-168. doi: 10.3310/hta10330. Health Technol Assess. 2006. PMID: 16959169
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.Health Technol Assess. 2006 Aug;10(28):iii-iv, xi-xiv, 1-183. doi: 10.3310/hta10280. Health Technol Assess. 2006. PMID: 16904047
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.Health Technol Assess. 2006 Mar;10(9):1-132. iii-iv. doi: 10.3310/hta10090. Health Technol Assess. 2006. PMID: 16545208
Cited by
-
The rise of artificial intelligence for cognitive behavioral therapy: A bibliometric overview.Appl Psychol Health Well Being. 2025 May;17(2):e70033. doi: 10.1111/aphw.70033. Appl Psychol Health Well Being. 2025. PMID: 40274359 Free PMC article. Review.
-
Cost Utility Analysis of Internet-Based Cognitive Behavioral Therapy for Major Depressive Disorder: Randomized Controlled Trial.J Med Internet Res. 2025 Feb 19;27:e67567. doi: 10.2196/67567. J Med Internet Res. 2025. PMID: 39970426 Free PMC article. Clinical Trial.
-
Global trends in depressive disorder prevalence and DALYs among young populations: a comprehensive analysis from 1990 to 2021.BMC Psychiatry. 2024 Dec 23;24(1):943. doi: 10.1186/s12888-024-06419-2. BMC Psychiatry. 2024. PMID: 39716116 Free PMC article.
References
-
- PAHO . The Burden of Mental Disorders. 2021. https://www.paho.org/en/enlace/burden-mental-disorders
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
