

The INFLUENCE 3.0 model: Updated predictions of locoregional recurrence and contralateral breast cancer, now also suitable for patients treated with neoadjuvant systemic therapy
- PMID: 39541608
- PMCID: PMC11605451
- DOI: 10.1016/j.breast.2024.103829
The INFLUENCE 3.0 model: Updated predictions of locoregional recurrence and contralateral breast cancer, now also suitable for patients treated with neoadjuvant systemic therapy
Abstract
Background: Individual risk prediction of 5-year locoregional recurrence (LRR) and contralateral breast cancer (CBC) supports decisions regarding personalised surveillance. The previously developed INFLUENCE tool was rebuild, including a recent population and patients who received neoadjuvant systemic therapy (NST).
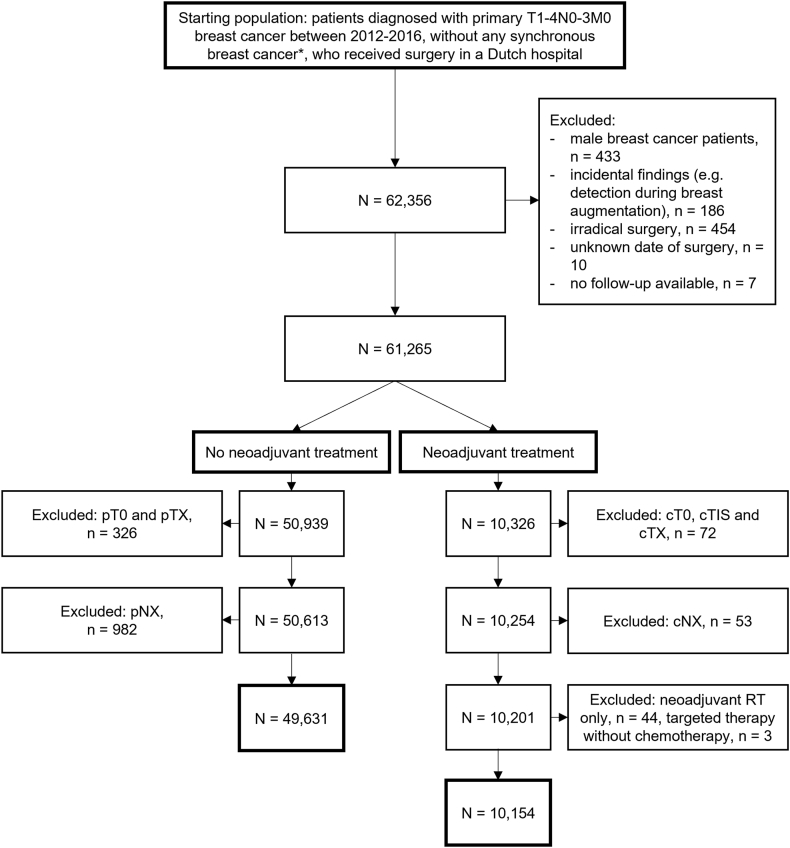
Methods: Women, surgically treated for nonmetastatic breast cancer, diagnosed between 2012 and 2016, were selected from the Netherlands Cancer Registry. Cox regression with restricted cubic splines was compared to Random Survival Forest (RSF) to predict five-year LRR and CBC risks. Separate models were developed for NST patients. Discrimination and calibration were assessed by 100x bootstrap resampling.
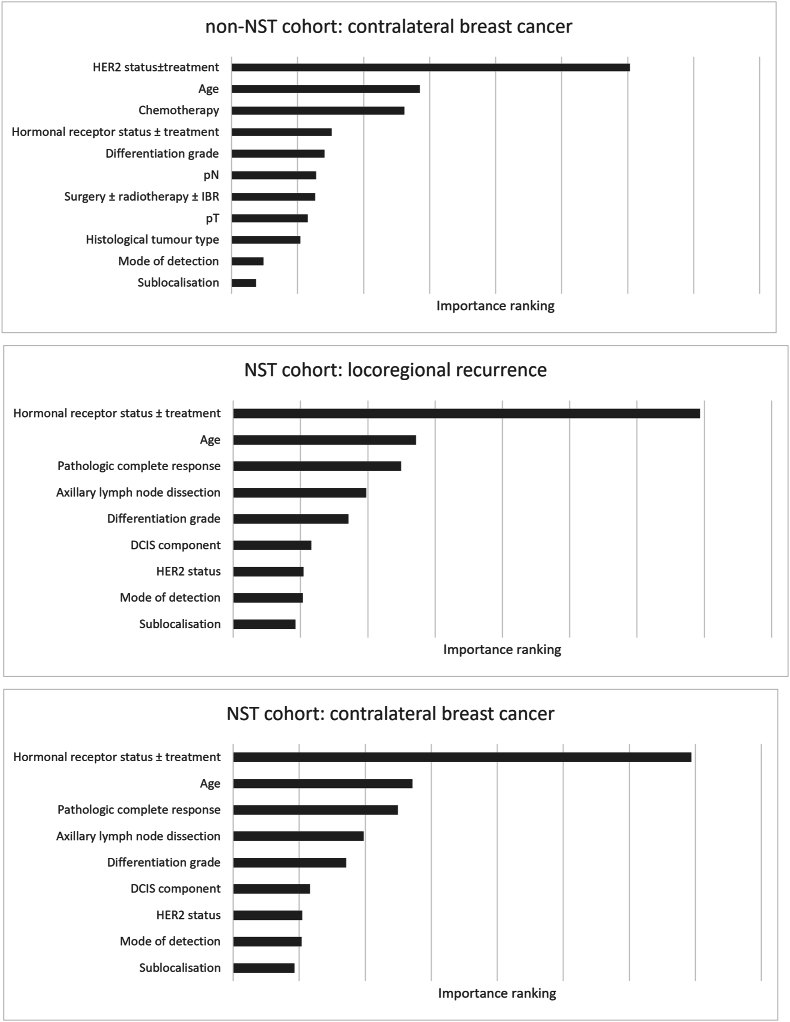
Results: In the non-NST and NST group, 49,631 and 10,154 patients were included, respectively. Age, mode of detection, histology, sublocalisation, grade, pT, pN, hormonal receptor status ± endocrine treatment, HER2 status ± targeted treatment, surgery ± immediate reconstruction ± radiation therapy, and chemotherapy were significant predictors for LRR and/or CBC in non-NST patients. For NST patients this was similar, but excluding (y)pT and (y)pN status, and including presence of ductal carcinoma in situ, axillary lymph node dissection and pathologic complete response. For non-NST patients, the Cox and RSF models were integrated in the online tool with 5-year AUCs of 0.77 (95%CI:0.77-0.77) and 0.68 (95%CI:0.67-0.68)] for LRR and CBC prediction, respectively. For NST patients, the RSF model performed best (AUCs 0.77 (95%CI:0.76-0.78) and 0.73 (95%CI:0.69-0.76) for LRR and CBC, respectively). Regarding calibration, observed-predicted differences were all <1 %.
Conclusion: This INFLUENCE 3.0 models showed moderate performance in LRR and CBC prediction. The models have been made available as online tool to enable clinical decision support regarding personalised follow-up.
Keywords: Breast cancer; Contralateral breast cancer; Follow-up; Locoregional recurrence; Prediction; Surveillance.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of coompeting interest Tom A. Hueting declares employment at Evidencio. The other authors declare no competing interests.
Figures

References
-
- Witteveen A., Vliegen I.M., Sonke G.S., Klaase J.M., Mj I.J., Siesling S. Personalisation of breast cancer follow-up: a time-dependent prognostic nomogram for the estimation of annual risk of locoregional recurrence in early breast cancer patients. Breast Cancer Res Treat. 2015;152(3):627–636. - PMC - PubMed
-
- van der Meer D.J., Kramer I., van Maaren M.C., van Diest P.J., S C.L., Maduro J.H., et al. Comprehensive trends in incidence, treatment, survival and mortality of first primary invasive breast cancer stratified by age, stage and receptor subtype in The Netherlands between 1989 and 2017. Int J Cancer. 2021;148(9):2289–2303. - PMC - PubMed
-
- Fang S.Y., Wang Y.L., Lu W.H., Lee K.T., Kuo Y.L., Fetzer S.J. Long-term effectiveness of an E-based survivorship care plan for breast cancer survivors: a quasi-experimental study. Patient Educ Couns. 2020;103(3):549–555. - PubMed
-
- Volkel V., Hueting T.A., Draeger T., van Maaren M.C., de Munck L., Strobbe L.J.A., et al. Improved risk estimation of locoregional recurrence, secondary contralateral tumors and distant metastases in early breast cancer: the INFLUENCE 2.0 model. Breast Cancer Res Treat. 2021;189(3):817–826. - PMC - PubMed
-
- Aalders K.C., van Bommel A.C., van Dalen T., Sonke G.S., van Diest P.J., Boersma L.J., et al. Contemporary risks of local and regional recurrence and contralateral breast cancer in patients treated for primary breast cancer. Eur J Cancer. 2016;63:118–126. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
