

CONNECT: Coordinating Options for Neurovascular Patients Needing Electrophysiology Consults and Treatments
- PMID: 39544275
- PMCID: PMC11559453
- DOI: 10.1177/19418744241289973
CONNECT: Coordinating Options for Neurovascular Patients Needing Electrophysiology Consults and Treatments
Abstract
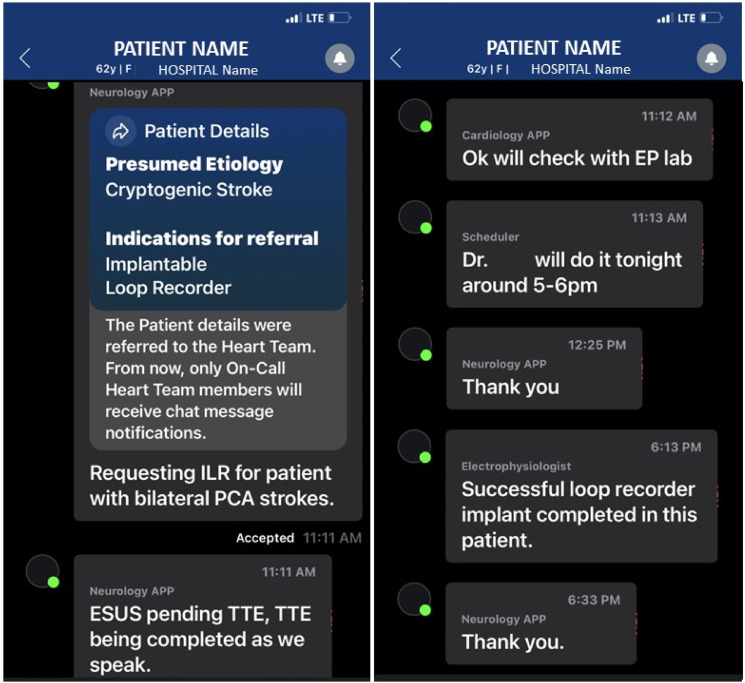
Background and purpose: Though Event Monitors (EM) and Implantable Loop Recorders (ILR) are prevalent in stroke workups, complex processes to obtain placement of these device might result in delays. Our aim was to determine if the CONNECT (Coordinating Options for Neurovascular patients Needing Electrophysiology Consults and Treatments) pathway could improve Stroke-to-Electrophysiology (EP) communications, increase EM and ILR device placements prior to discharge, shorten placement time, and preserve satisfaction.
Methods: We assessed device placements when an EP consult was obtained [Pre-CONNECT (5/1/21-4/30/22), CONNECT (5/1/22-4/30/23)] for patients with stroke. In the Pre- period, consults were sent via EPIC electronic medical record (EMR), with additional direct communication when desired. In the CONNECT period, the pathway and module allowed for immediate communication between services. Outcomes included case rate, times, length of stay, and satisfaction. Hospital reports detailed Order to Activation (O-A) days. EM report review was used to obtain O-A time. Clinician satisfaction was assessed using Qualtrics survey. Patient satisfaction was assessed with Hospital Consumer Assessment of Health care Clinicians and Systems (HCAHPS) survey. Man-Whitney U test was used.
Results: 78 patients were included (30EM(38.5%), 48ILR(61.5%)). Age was 68 years (P = 0.58). For ILRs, inpatient placements prior to discharge increased (3Pre vs 51 CONNECT; P < 0.0001) as did outpatient placements (5 vs 16; P = 0.02). Order to Activation (O-A) time savings were significant for ILR overall (32 days vs 1 day; P = 0.03) and for Inpatient EM (13 days vs 3 days; P = 0.003). Time for consultant to view was 4 min and to respond was 6 min. Devices were placed at a median 6 hrs 32 min (EM: 4 hrs 19 min; ILR:7 hrs36 min). All (12/12) clinicians preferred the technique. Patient satisfaction improved on 13/19 (68%) questions.
Conclusions: There was a 1600% increase in ILR placements prior to discharge that was associated with the time period that the CONNECT process was in place. The robust improvement in ILR placements prior to discharge, high satisfaction, ease of use, closed loop communication, and respect for autonomy allowing more organic parallel discussions with patients improved clinician workflow which could potentially improve future risk reduction strategies.
Keywords: atrial fibrillation; electrophysiology; implantable loop recorders; stroke.
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Immediate implantable loop recorder implantation for detecting atrial fibrillation in cryptogenic stroke.J Stroke Cerebrovasc Dis. 2023 Mar;32(3):106988. doi: 10.1016/j.jstrokecerebrovasdis.2023.106988. Epub 2023 Jan 14. J Stroke Cerebrovasc Dis. 2023. PMID: 36645969
-
The utility of implantable loop recorders in patient management: an age- and indication-stratified study in the outpatient-implant era.Eur Heart J Qual Care Clin Outcomes. 2022 Oct 26;8(7):770-777. doi: 10.1093/ehjqcco/qcab071. Eur Heart J Qual Care Clin Outcomes. 2022. PMID: 34601557
-
Effectiveness, utilisation and cost associated with implantable loop recorders versus external monitors after ischaemic or cryptogenic stroke.Open Heart. 2024 May 8;11(1):e002714. doi: 10.1136/openhrt-2024-002714. Open Heart. 2024. PMID: 38719499 Free PMC article.
-
Implantable Loop Recorders for Cryptogenic Stroke (Plus Real-World Atrial Fibrillation Detection Rate with Implantable Loop Recorders).Card Electrophysiol Clin. 2018 Mar;10(1):111-118. doi: 10.1016/j.ccep.2017.11.011. Card Electrophysiol Clin. 2018. PMID: 29428132
-
Implantable loop recorders in patients with atrial fibrillation.Expert Rev Cardiovasc Ther. 2022 Dec;20(12):919-928. doi: 10.1080/14779072.2022.2153673. Expert Rev Cardiovasc Ther. 2022. PMID: 36444859 Review.
References
-
- Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: stroke Prevention in Atrial Fibrillation III randomised clinical trial. Lancet. 1996;348(9028):633-638. - PubMed
-
- Brachmann J, Morillo CA, Sanna T, et al. Uncovering atrial fibrillation beyond short-term monitoring in cryptogenic stroke patients: three-year results from the cryptogenic stroke and underlying atrial fibrillation trial. Circ Arrhythm Electrophysiol. 2016;9(1):e003333. doi:10.1161/circep.115.003333 - DOI - PubMed
LinkOut - more resources
Full Text Sources