

Seroprevalence and silent infection rate during SARS-CoV-2 pandemic among children and adolescents in Western Pomerania: a multicenter, cross-sectional study-the COVIDKID study
- PMID: 39544417
- PMCID: PMC11562825
- DOI: 10.7717/peerj.18384
Seroprevalence and silent infection rate during SARS-CoV-2 pandemic among children and adolescents in Western Pomerania: a multicenter, cross-sectional study-the COVIDKID study
Abstract
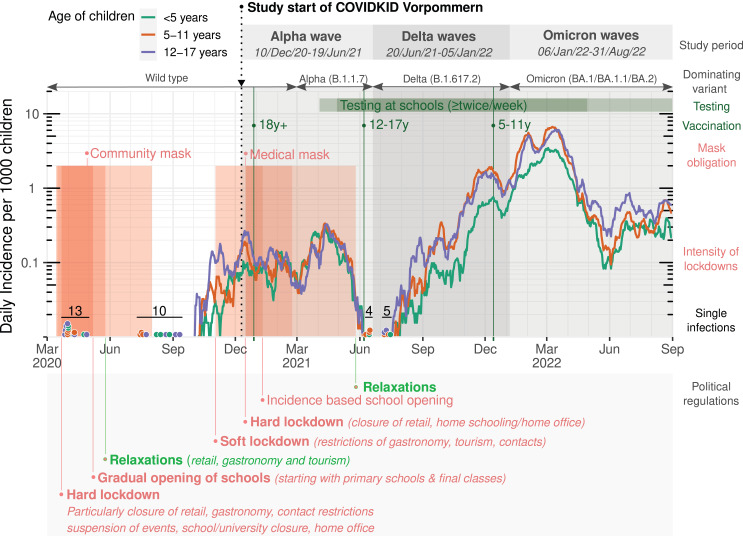
Background: Limited data on SARS-CoV-2 seroprevalence in rural areas of northern Germany necessitate comprehensive cohort studies. We aimed to evaluate the seroprevalence, silent infection (SI) rates and risk factors for infections among children and adolescents in Western Pomerania from December 2020 to August 2022.
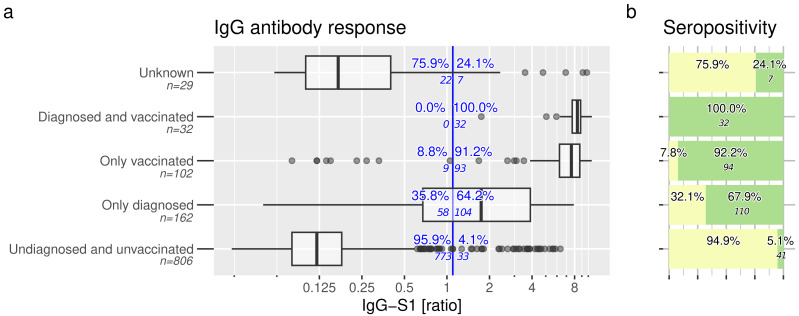
Methods: In this cross-sectional study, serum or plasma samples from children and adolescents (6 months to 17 years) were collected during routine blood draw. SARS-CoV-2 specific antibodies (S1 and nucleocapsid) and their neutralizing capacity were analyzed using commercially available enzyme-linked immunosorbent and neutralization assays. Socio-demographic data and information about SARS-CoV-2 infection or vaccination were obtained. Multivariable logistic regression was used to identify independent risk factors for SARS-CoV-2 infections and SI.
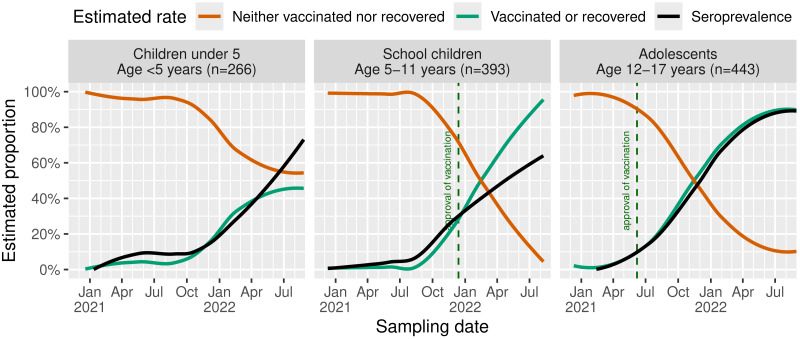
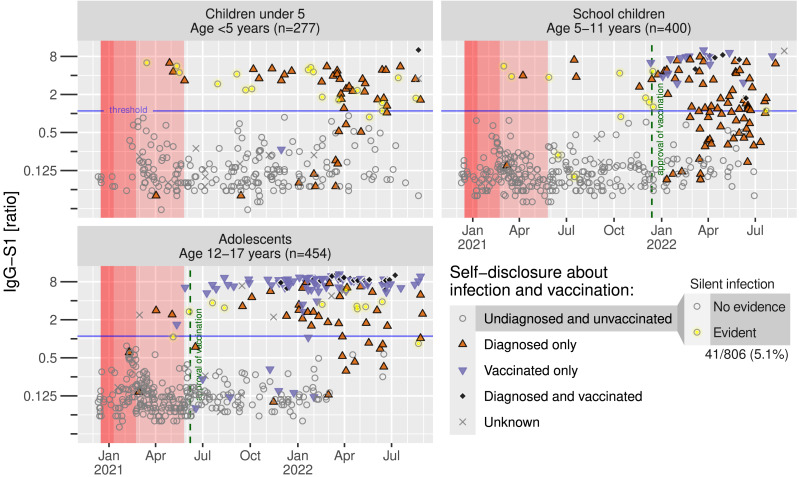
Results: A total of 1,131 blood samples were included into the study. Overall, SARS-CoV-2 seroprevalence was 25.1%, strongly influenced by the pandemic course, predominant virus variants, age and approval of vaccination. SI rate was 5.4% (95%-CI [3.7%-6.8%]) among unvaccinated and undiagnosed children over the entire study period with highest rates among adolescents. Main risk factor despite the time at risk for silent infections was an infected household member (Odds ratio = 9.88, 95%-CI [4.23-22.9], p < 0.001). Factors associated with overall infections (known and silent) also include the infection of a household member (Odds ratio = 17.8, 95%-CI [10.7-29.6], p < 0.001).
Conclusions: We believe that the introduction of governmental measures and systematic test strategies in schools strongly impacted on the SI rate, as we suspect that asymptomatic cases have already been identified, resulting in surprisingly low SI identified in our study.
Keywords: Covid-19; IgA-S1; IgG-S1; NCP-IgG; Pandemic; Pediatric; SARS-CoV-2; Serology; Seroprevalence; Silent infection.
©2024 Vollmer et al.
Conflict of interest statement
Almut Meyer-Bahlburg received funding for the project by the Ministry for Economics, Labour and Health Mecklenburg-Vorpommern. Lars Kaderali was a member of the Corona Expert Council advising the Federal Government of Germany.
Figures

References
-
- Almeida Carvalho JM, Camargo CN, De Souza Luna LK, Rabha AC, Conte DD, Mariano RF, De Oliveira Junior FI, Barbosa GR, Moreira LVL, Chaves APC, Perosa AH, Bellei N. Household transmission of COVID-19 according to index case: children, parents, and healthcare workers. Brazilian Journal of Microbiology. 2022;53:1345–1348. doi: 10.1007/s42770-022-00762-w. - DOI - PMC - PubMed
-
- Anzalone AJ, Sun J, Vinson AJ, Beasley WH, Hillegass WB, Murray K, Hendricks BM, Haendel M, Geary CR, Bailey KL, Hanson CK, Miele L, Horswell R, McMurry JA, Porterfield JZ, Vest MT, Bunnell HT, Harper JR, Price BS, Santangelo SL, Rosen CJ, McClay JC, Hodder SL. Community risks for SARS-CoV-2 infection among fully vaccinated US adults by rurality: a retrospective cohort study from the National COVID Cohort Collaborative. PLOS ONE. 2023;18:e0279968. doi: 10.1371/journal.pone.0279968. - DOI - PMC - PubMed
-
- Bignami-Van Assche S, Ferraccioli F, Riccetti N, Gomez-Ramirez J, Ghio D, Stilianakis NI. Urban-rural disparities in COVID-19 hospitalisations and mortality: a population-based study on national surveillance data from Germany and Italy. PLOS ONE. 2024;19:e0301325. doi: 10.1371/journal.pone.0301325. - DOI - PMC - PubMed
-
- Boey L, Roelants M, Merckx J, Hens N, Desombere I, Duysburgh E, Vandermeulen C. Age-dependent seroprevalence of SARS-CoV-2 antibodies in school-aged children from areas with low and high community transmission. European Journal of Pediatrics. 2022;181:571–578. doi: 10.1007/s00431-021-04222-9. - DOI - PMC - PubMed
-
- Brinkmann F, Diebner HH, Matenar C, Schlegtendal A, Eitner L, Timmesfeld N, Maier C, Lücke T. Seroconversion rate and socio-economic and ethnic risk factors for SARS-CoV-2 infection in children in a population-based cohort, Germany, 2020 to 2021. Eurosurveillance. 2022;27:2101028. doi: 10.2807/1560-7917.ES.2022.27.37.2101028. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
