

Vitamin D association with systemic sclerosis and its clinical features: A systematic review, meta-analysis, and meta-regression
- PMID: 39544900
- PMCID: PMC11559530
- DOI: 10.1177/23971983241288591
Vitamin D association with systemic sclerosis and its clinical features: A systematic review, meta-analysis, and meta-regression
Abstract
Objectives: The aim of this review was to summarize existing data on the contribution of Vitamin D level and/or deficiency/insufficiency to systemic sclerosis susceptibility and its clinical features.
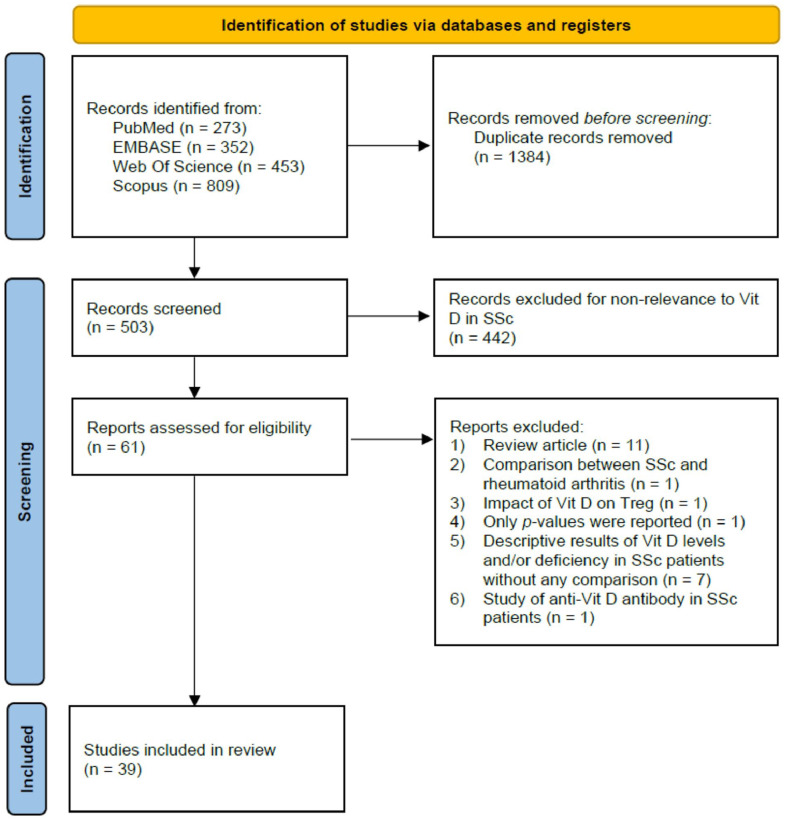
Methods: An electronic literature search for eligible studies among all papers published prior to 30 June 2024 was conducted through PubMed, EMBASE, Web of science, and Scopus databases. Meta-analyses estimating pooled raw mean differences, odds ratios, and Pearson r together with subgroup analyses and meta-regressions were performed for the association of Vitamin D with susceptibility to systemic sclerosis and disease presentation.
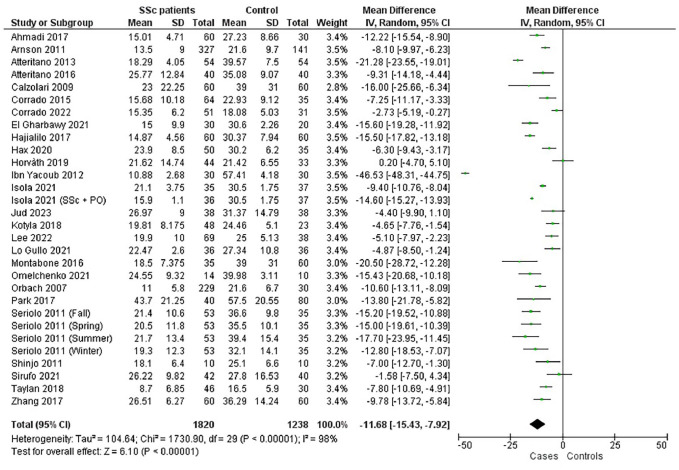
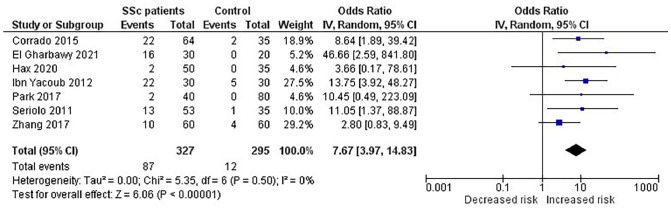
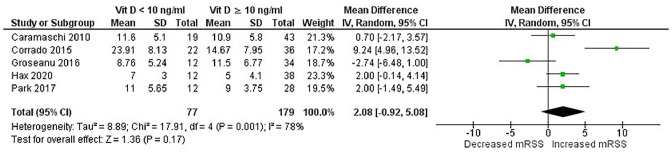
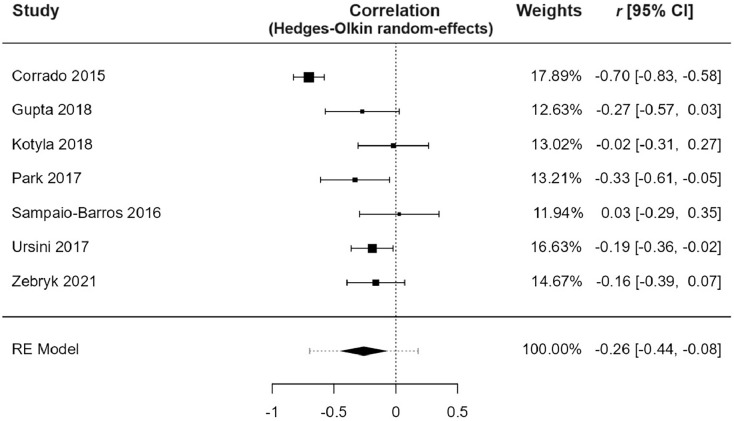
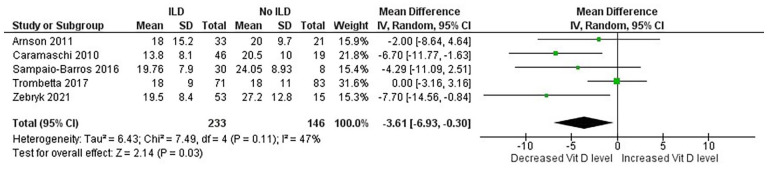
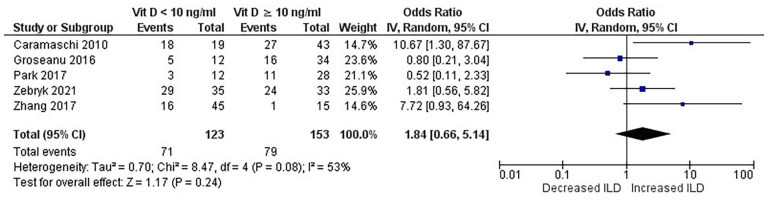
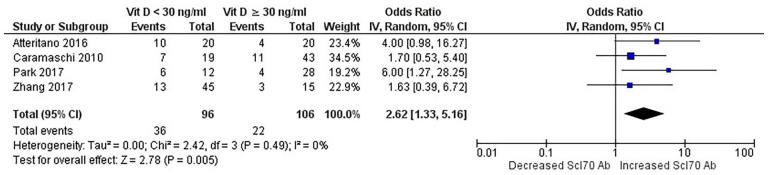
Results: Combined analysis revealed a significant decrease in Vitamin D level in systemic sclerosis patients comparatively to healthy controls, with raw mean differences 95% CI = -11.68 [-15.43 to -7.92] ng/mL, p < 1 E-10. Likewise, Vitamin D insufficiency (Vitamin D < 30 ng/mL) and deficiency (<10 ng/mL) were significantly associated with systemic sclerosis; odds ratios 95% CI = 3.58 [2.59-4.95], p < 1 E-10 and odds ratios 95% CI = 7.67 [3.97-14.83], p < 1 E-10, respectively. Moreover, decreased Vitamin D level was significantly associated with interstitial lung disease occurrence (raw mean differences 95% CI = -3.61 [-6.93 to -0.3], p = 0.003), while Vitamin D deficiency was associated with increased systolic pulmonary arterial pressure, raw mean differences (95% CI = 4.17 [1.44-6.89], p = 0.003). Besides, Vitamin D level was negatively correlated with the modified Rodnan skin score, r (95% CI = -0.26 [-0.44 to -0.08], p = 0.004). Conversely, Vitamin D level was significantly increased in systemic sclerosis patients with cutaneous calcinosis, raw mean differences (95% CI = 4.18 [1.07-7.28], p = 0.008).
Conclusion: This meta-analysis showed that decreased Vitamin D level was associated with susceptibility to systemic sclerosis, interstitial lung disease occurrence, increased systolic pulmonary arterial pressure, and higher modified Rodnan skin score. Conversely, calcinosis was found to be associated with increased Vitamin D level.
Registration: This review has been registered on PROSPERO: CRD42024565045, available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024565045.
Keywords: Systemic sclerosis; Vitamin D; meta-analysis; meta-regression; systematic review.
© The Author(s) 2024.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report that there are no competing interests to declare. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Figures






Similar articles
-
Association between vitamin D status and thyroid cancer: a meta-analysis.Front Nutr. 2024 Jun 18;11:1423305. doi: 10.3389/fnut.2024.1423305. eCollection 2024. Front Nutr. 2024. PMID: 38962442 Free PMC article.
-
Association of 10 Polymorphisms in PLA2R1 and HLA DQA1 Genes with Primary Membranous Nephropathy Risk: A Meta-Analysis and a Meta-Regression.Biomark Insights. 2024 Jun 10;19:11772719241259602. doi: 10.1177/11772719241259602. eCollection 2024. Biomark Insights. 2024. PMID: 38863528 Free PMC article.
-
Vitamin D levels in systemic sclerosis patients: a meta-analysis.Drug Des Devel Ther. 2017 Oct 27;11:3119-3125. doi: 10.2147/DDDT.S144860. eCollection 2017. Drug Des Devel Ther. 2017. PMID: 29138534 Free PMC article. Review.
-
Association of HLA class II alleles and haplotypes with bullous and mucus membrane pemphigoid risk: A systematic review, a meta-analysis and a meta-regression.Int J Immunopathol Pharmacol. 2024 Jan-Dec;38:3946320241296903. doi: 10.1177/03946320241296903. Int J Immunopathol Pharmacol. 2024. PMID: 39442009 Free PMC article.
-
The effect of vitamin D deficiency during pregnancy on adverse birth outcomes in neonates: a systematic review and meta-analysis.Front Pediatr. 2024 May 14;12:1399615. doi: 10.3389/fped.2024.1399615. eCollection 2024. Front Pediatr. 2024. PMID: 38808102 Free PMC article.
Cited by
-
Vitamin D and Its Role in Rheumatic Diseases.Metabolites. 2025 Apr 9;15(4):259. doi: 10.3390/metabo15040259. Metabolites. 2025. PMID: 40278388 Free PMC article. Review.
References
-
- Bellando-Randone S, Matucci-Cerinic M. Very Early systemic sclerosis and pre-systemic sclerosis: definition, recognition, clinical relevance and future directions. Curr Rheumatol Rep 2017; 19(10): 65. - PubMed
-
- Matucci-Cerinic M, Kahaleh B, Wigley FM. Review: evidence that systemic sclerosis is a vascular disease. Arthritis Rheum 2013; 65(8): 1953–1962. - PubMed
-
- Rezaei R, Aslani S, Dashti N, et al.. Genetic implications in the pathogenesis of systemic sclerosis. Int J Rheum Dis 2018; 21(8): 1478–1486. - PubMed
Publication types
LinkOut - more resources
Full Text Sources