

Treatment of thoracic outlet syndrome to relieve chronic migraine
- PMID: 39545467
- PMCID: PMC11925132
- DOI: 10.1002/ca.24242
Treatment of thoracic outlet syndrome to relieve chronic migraine
Abstract
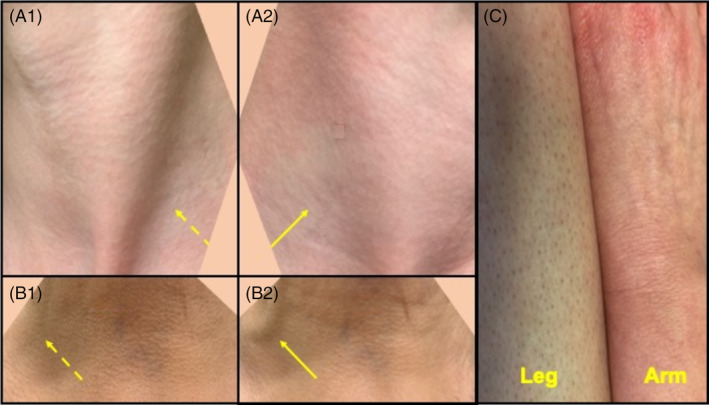
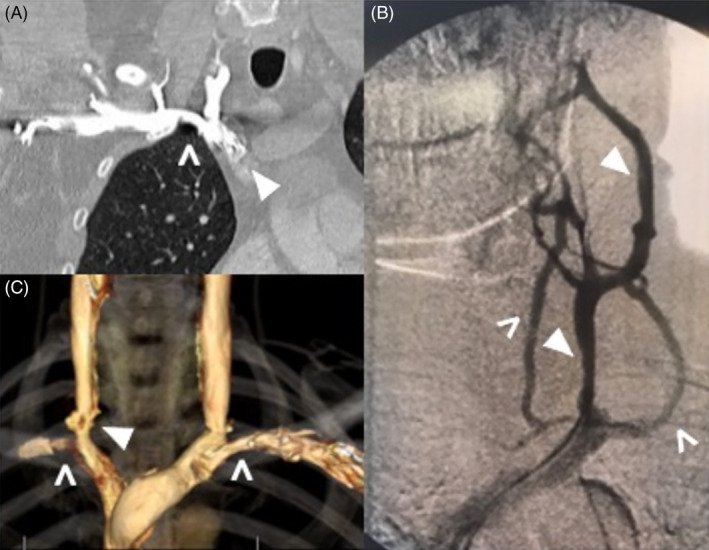
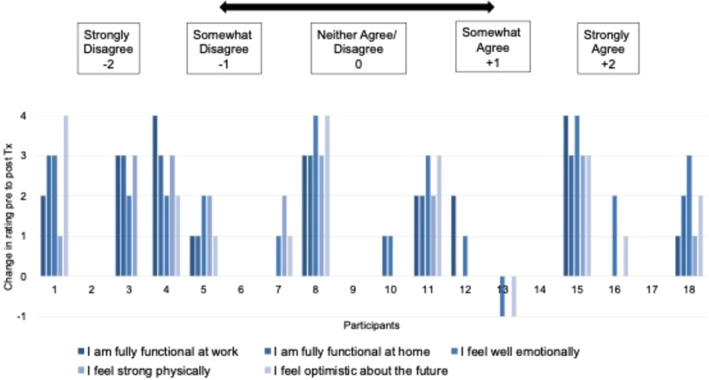
Prior case reports have suggested that treating thoracic outlet syndrome (TOS) may relieve intractable migraine headaches, but there has been no case series large enough to show when underlying TOS should be suspected as a contributor to migraine burden. This observational followed by questionnaire study was performed in an outpatient neurology practice to identify clinical features of patients with migraine in which TOS contributed to migraine burden. We report the clinical features of 50 consecutive patients (48 women, 2 men, age = 43.9+/12.7 years) who were treated for chronic migraine and TOS (20 migraine with aura, 28 migraine without aura, two hemiplegic migraines). Headaches had become chronic within 1 year of onset in 21 patients (42%) with characteristics as follows (percentages are based on known data): greater severity ipsilateral to TOS limb pain (38/50=76%), presence of limb swelling (32/48=67%), and worsened by recumbency (32/38=84%). Thirty-two patients eventually needed surgery, which included percutaneous transluminal venoplasty, 1st rib removal, scalenectomy, pectoralis minor tenotomy, and/or vein patching. The mean improvement of headaches on the treated side was 72 ± 26.7%; 12 patients experienced complete resolution of headaches after treatment of TOS (follow-up 7.2 ± 5.2 months). Questionnaire responders reported significant reductions in headache days (18.3 ± 8.6 to 11.1 ± 10.8 days/month, p < 0.0016), severity (7.8+/2.5 to 5.4 ± 2.9, p < 0.00079), and need for emergency care (3.6 ± 4.0 to 0.71 ± 1.3 visits/year, p < 0.0029). Chronic migraines can be important manifestations of TOS. Early transition to a chronic state, lateralized limb pain, and headaches worsened by recumbency are clues to the contribution of TOS pathology. Addressing the TOS contribution to migraine can significantly reduce migraine headache burden.
Keywords: brachial plexus; headache; migraine; subclavian vein; thoracic outlet syndrome.
© 2024 The Author(s). Clinical Anatomy published by Wiley Periodicals LLC on behalf of American Association of Clinical Anatomists and British Association of Clinical Anatomists.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Botulinum toxins for the prevention of migraine in adults.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD011616. doi: 10.1002/14651858.CD011616.pub2. Cochrane Database Syst Rev. 2018. PMID: 29939406 Free PMC article.
-
Preventive drug treatments for adults with chronic migraine: a systematic review with economic modelling.Health Technol Assess. 2024 Oct;28(63):1-329. doi: 10.3310/AYWA5297. Health Technol Assess. 2024. PMID: 39365169 Free PMC article.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Symptomatic treatment of migraine in children: a systematic review of medication trials.Pediatrics. 2005 Aug;116(2):e295-302. doi: 10.1542/peds.2004-2742. Pediatrics. 2005. PMID: 16061583
References
-
- Ahn, S. S. , Miller, T. J. , Chen, J. F. , Chen, S. W. , Feldtman, R. , & Hwang, W. (2013). Internal jugular vein stenosis in patients with thoracic outlet symptoms. Journal of Vascular Surgery, 57, 100S.
-
- Akobo, S. , & Tubbs, R. S. (2020). Superior Petrosal Sinus. In Tubbs R. S. (Ed.), Anatomy, imaging and surgery of the intracranial dural venous sinuses (pp. 117–124). Elsevier.
-
- Balachandra, N. , Padmalatha, K. , Prakash, B. , & Ramesh, B. (2012). Variation of the veins of the head and neck‐external jugular and facial vein. International Journal of Anatomical Variations, 5, 99–101.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
