

Key Takeaways From the ISASS Webinar Series on Current and Emerging Techniques in Endoscopic Spine Surgery | Part 2: Polytomous Rasch Analysis of Learning Curve and Surgeon Endorsement of Biportal, Interlaminar, and Transforaminal Endoscopic Stenosis Decompression, Discectomy, and Laminectomy in Combination With Interspinous Process Spacers
- PMID: 39547677
- PMCID: PMC11616440
- DOI: 10.14444/8673
Key Takeaways From the ISASS Webinar Series on Current and Emerging Techniques in Endoscopic Spine Surgery | Part 2: Polytomous Rasch Analysis of Learning Curve and Surgeon Endorsement of Biportal, Interlaminar, and Transforaminal Endoscopic Stenosis Decompression, Discectomy, and Laminectomy in Combination With Interspinous Process Spacers
Abstract
Background: The International Society for the Advancement of Spine Surgery hosted the second of a series of 4 webinars on endoscopic spine surgery techniques. The second webinar focused on the application of unilateral biportal endoscopy for discectomy and laminectomy in combination with interbody fusion and interspinous process spacers. This series was intended to identify current trends with contemporary modern endoscopic spine surgery techniques.
Objective: To analyze the level of surgeon endorsement for the presented endoscopic spine surgery techniques before and after the webinar utilizing polytomous Rasch analysis, as well as to evaluate the potential for these insights to inform clinical guideline recommendations.
Methods: A survey was available to 667 potential respondents during the Zoom webinar, collecting data on surgeon endorsements using a Likert scale. The polytomous Rasch model was employed to analyze responses while considering the complexity of decisions against surgeon expertise, developing a logarithmic measurement scale, allowing objective statistical analysis of categorical variables, highlighting incongruent or out of order items vs congruent and in order items, and driving improvement in clinical guidelines.
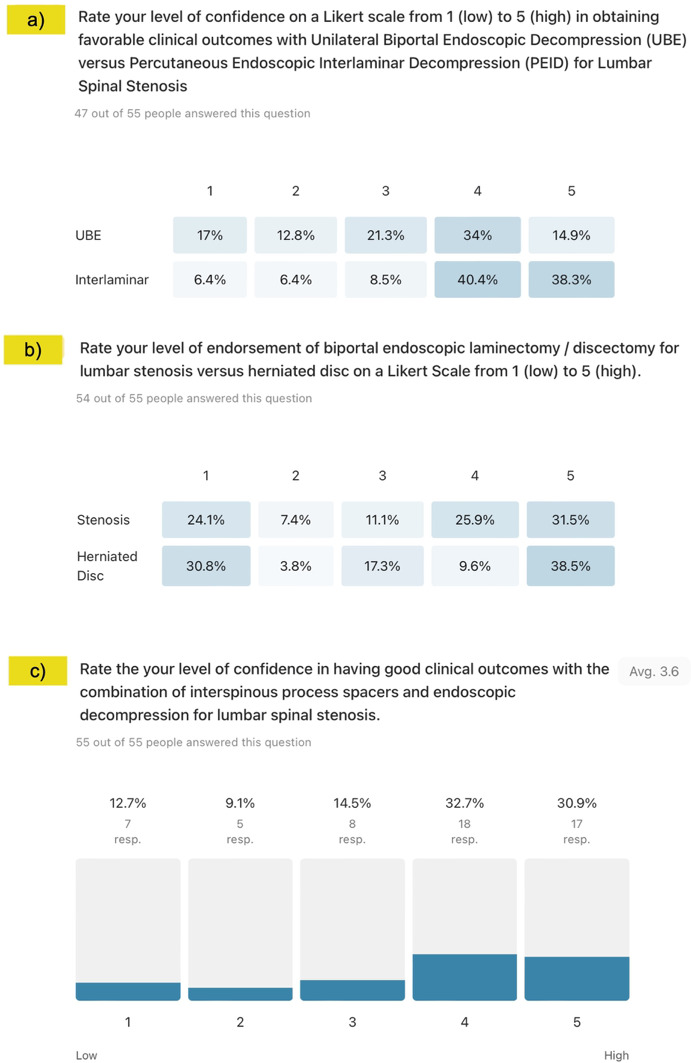
Results: Of the 667 surgeons who participated in the webinar, 224 accessed, 122 started, and 61 completed the prewebinar survey, achieving a 50.0% completion rate. Respondents comprised primarily orthopedic surgeons (70.5%) and neurosurgeons (24.6%), with fellows and medical students each making up 1.6%. These surgeons estimated that mastering the learning curve of endoscopic spine surgery required an average of 18.08 cases corroborated by postwebinar responses averaging 15.78 cases. Descriptive statistics revealed an acknowledgment of a learning curve in mastering endoscopic spine surgery, with a slight increase in recognition postwebinar (81.8% up from 80.3%). The data underscored the importance of cadaver courses and high-volume surgical practice before the webinar and highlighted the value of mentorship afterward, indicating a preference shift toward more interactive learning. The confidence in various endoscopic techniques saw notable changes, particularly for procedures involving interlaminar lateral canal decompression and the combined use of transforaminal endoscopic decompression with interspinous process spacers, which saw an increase in high-level endorsements postwebinar. Polytomous Rasch analysis provided insights into training methods and procedural techniques, with mentorship and cadaver courses emerging as key elements for mastering the learning curve. The analysis also highlighted a general consensus on the effectiveness of percutaneous endoscopic interlaminar decompression for lateral canal stenosis, reflecting evolving surgeon preferences and consensus on best practices. Infit and outfit statistics from the Rasch analysis suggested a good fit between the survey responses and the Rasch model both before and after the webinar, indicating minimal data distortion due to bias. Differential item functioning analysis showed no significant bias in item responses between orthopedic surgeons and neurosurgeons in the prewebinar survey, but it identified potential bias for one item postwebinar-unilateral biportal endoscopic laminectomy for central stenosis.
Conclusion: This webinar highlighted the importance of hands-on training methods such as cadaver courses and mentorship in mastering the complex spinal endoscopy procedures. The application of polytomous Rasch analysis provided a detailed understanding of surgeons' current preferences and perceptions, as well as the evolving consensus on best practices in endoscopic spine surgery, displaying wide acceptance of the percutaneous interlaminar endoscopic decompression for lateral canal stenosis decompression and a growing interest in integrating endoscopic techniques for more comprehensive spinal care, including wide decompression and spinal stabilization.
Clinical relevance: Assessing surgeon confidence and acceptance of endoscopic spinal surgeries using polytomous Rasch analysis.
Level of evidence: Level 2 (inferential) and 3 (observational) evidence because Rasch analysis provides statistical validation of instruments rather than direct clinical outcomes.
Keywords: clinical guidelines; discectomy; endoscopic spine surgery; interspinous process spacers (ISP); laminectomy; learning curve; percutaneous endoscopic interlaminar decompression (PEID); polytomous Rasch analysis; surgeon endorsement; unilateral biportal endoscopy (UBE).
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests : The authors declare no conflict of interest relevant to this research, and there was no personal circumstance or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. This research was not compiled to enrich anyone.
Figures










References
LinkOut - more resources
Full Text Sources
Research Materials