

The Financial Impact of Post Intensive Care Syndrome
- PMID: 39547719
- PMCID: PMC11681988
- DOI: 10.1016/j.ccc.2024.08.003
The Financial Impact of Post Intensive Care Syndrome
Abstract
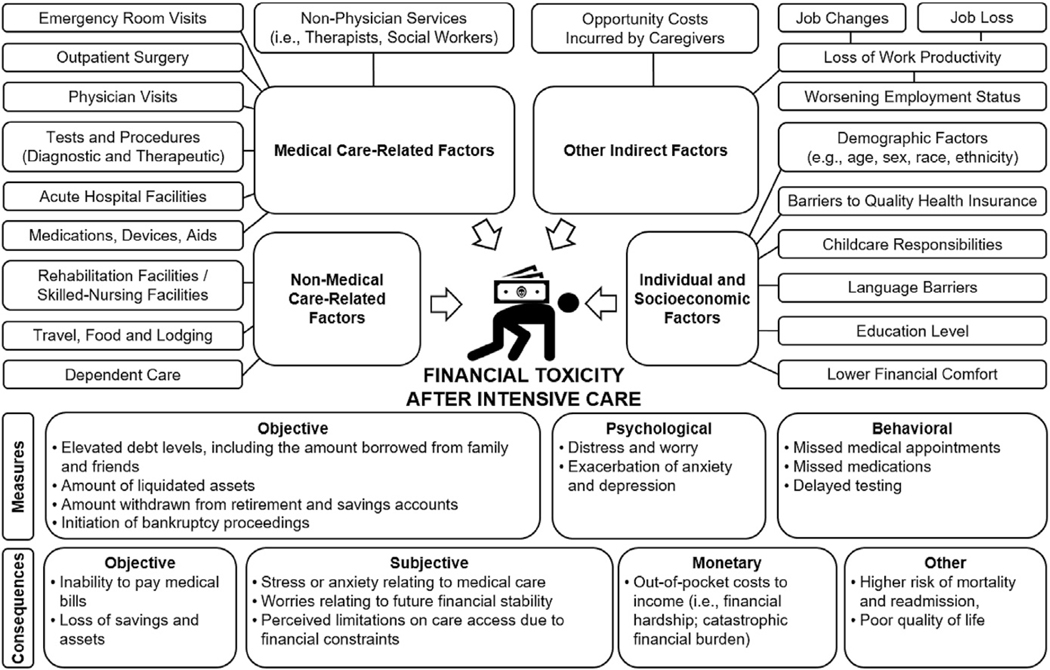
This review explores the financial consequences that survivors of critical illness often face following hospitalization in an intensive care unit (ICU). As part of the "post-intensive care syndrome" (PICS), these survivors often experience, in addition to physical and emotional challenges of PICS, major financial burdens resulting from their prolonged ICU treatments. The escalating costs of ICU care, coupled with the potential long-term effects on survivors' ability to work and maintain financial stability, have brought financial toxicity to the forefront of health care discussions. The current review examines the causes and consequences of financial toxicity.
Keywords: Critical illness; Employment; Financial burden; Intensive care unit.
Copyright © 2024 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The effectiveness of interventions to meet family needs of critically ill patients in an adult intensive care unit: a systematic review update.JBI Database System Rev Implement Rep. 2016 Mar;14(3):181-234. doi: 10.11124/JBISRIR-2016-2477. JBI Database System Rev Implement Rep. 2016. PMID: 27532144
-
Early intervention (mobilization or active exercise) for critically ill adults in the intensive care unit.Cochrane Database Syst Rev. 2018 Mar 27;3(3):CD010754. doi: 10.1002/14651858.CD010754.pub2. Cochrane Database Syst Rev. 2018. PMID: 29582429 Free PMC article.
-
Feasibility challenges in protein supplementation research: Insights from the convalescence of functional outcomes after intensive care unit stay in a Randomised Controlled Trial.Clin Nutr. 2025 Mar;46:119-130. doi: 10.1016/j.clnu.2025.01.020. Epub 2025 Jan 21. Clin Nutr. 2025. PMID: 39914233 Clinical Trial.
-
The Cleveland Clinic Post-ICU Recovery Clinic: Early Experience During the COVID-19 Pandemic.J Intensive Care Med. 2025 Aug;40(8):893-901. doi: 10.1177/08850666251326551. Epub 2025 Mar 23. J Intensive Care Med. 2025. PMID: 40123228
-
Critical illness survivors' experiences of attending an intensive care unit follow-up service: a systematic review protocol.JBI Evid Synth. 2023 Dec 1;21(12):2438-2445. doi: 10.11124/JBIES-23-00132. JBI Evid Synth. 2023. PMID: 37661769
Cited by
-
Translation and validation of the Chinese version of the post-intensive care syndrome questionnaire.BMC Nurs. 2025 Jul 11;24(1):906. doi: 10.1186/s12912-025-03576-x. BMC Nurs. 2025. PMID: 40646508 Free PMC article.
-
Efficacy of Combined Use of PELNAC and Platelet-rich Plasma in Promoting Wound Healing.Plast Reconstr Surg Glob Open. 2025 Aug 6;13(8):e7062. doi: 10.1097/GOX.0000000000007062. eCollection 2025 Aug. Plast Reconstr Surg Glob Open. 2025. PMID: 40771260 Free PMC article.
References
-
- Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med 2012;40(2):502–9. - PubMed
-
- Schwitzer E, Jensen KS, Brinkman L, et al. Survival ≠ recovery: a narrative review of post-intensive care syndrome. Chest Critical Care 2023;1(1):100003.
-
- Harvey MA, Davidson JE. Postintensive care syndrome: right care, right now… and later. Crit Care Med 2016;44(2):381–5. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
