

Effectiveness of treat-to-target cholesterol-lowering interventions on cardiovascular disease and all-cause mortality risk in the community-dwelling population: a target trial emulation
- PMID: 39548082
- PMCID: PMC11568141
- DOI: 10.1038/s41467-024-54078-4
Effectiveness of treat-to-target cholesterol-lowering interventions on cardiovascular disease and all-cause mortality risk in the community-dwelling population: a target trial emulation
Abstract
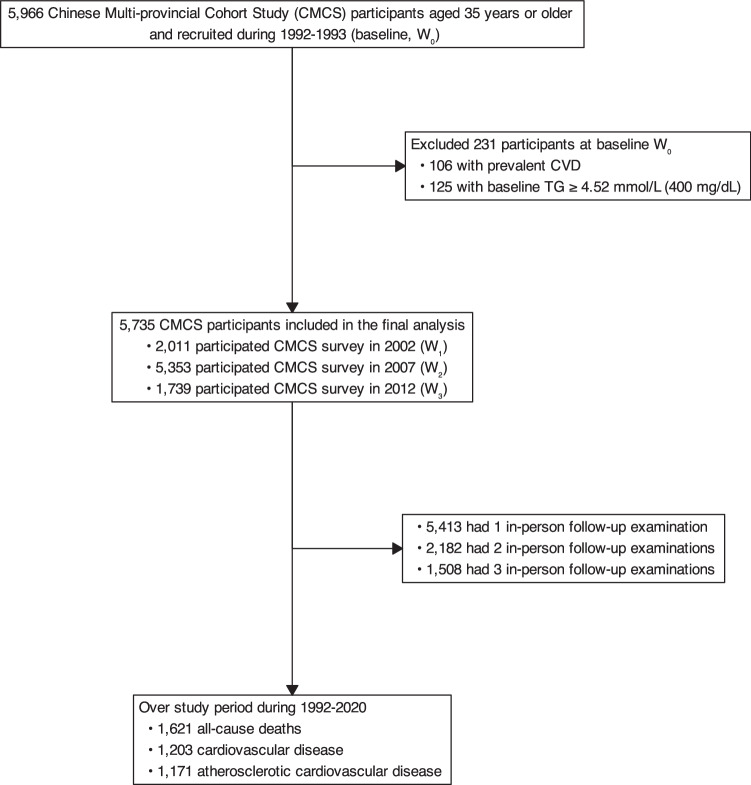
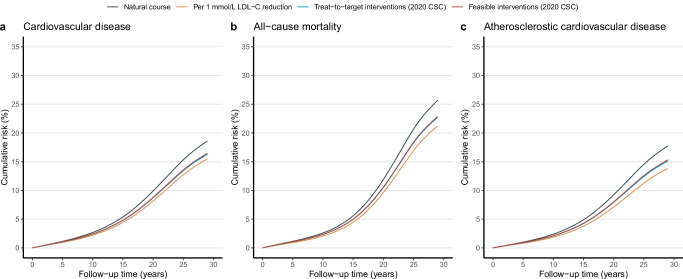
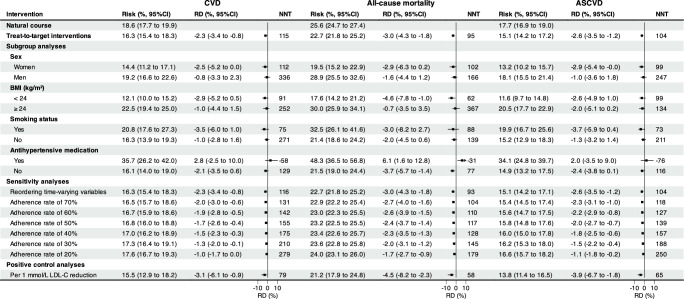
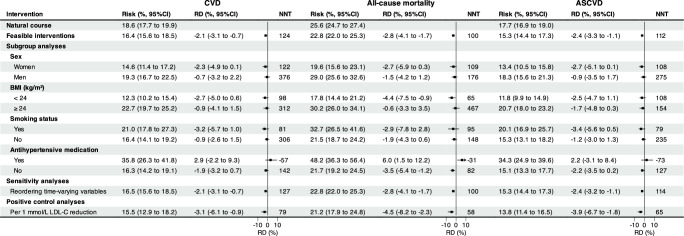
Little is known about the long-term effectiveness of risk-based treat-to-target cholesterol-lowering interventions on cardiovascular risk. Here, we show the emulated effectiveness of guideline-recommended low-density and non-high-density lipoprotein cholesterol-lowering interventions using the absolute risk reduction (ARR) and the restricted mean event-free time-based number needed to treat (NNT). With 5,375 participants, the 29-year risks for cardiovascular disease (CVD), all-cause mortality, and atherosclerotic CVD were 18.6%, 25.6%, and 17.7%, respectively. Long-term treat-to-target interventions showed significant reductions in CVD (ARR -2.3%, 95%CI -3.4% to -0.8%; NNT 115), all-cause mortality (-3.0%, -4.3% to -1.8%; 95), and atherosclerotic CVD (-2.6%, -3.5% to -1.2%; 104). Such effects appear more pronounced in women, smokers, and those with body mass index < 24 kg/m² or higher adherence rates.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
-
- Chinese Society of Cardiology of Chinese Medical Association, Cardiovascular Disease Prevention and Rehabilitation Committee of Chinese Association of Rehabilitation Medicine, Cardiovascular Disease Committee of Chinese Association of Gerontology and Geriatrics, Thrombosis Prevention and Treatment Committee of Chinese Medical Doctor Association. Chinese Guideline on the Primary Prevention of Cardiovascular Diseases. Cardiol. Discov. 1, 70–104 (2021).
-
- Brandts, J. & Ray, K. K. Novel and future lipid-modulating therapies for the prevention of cardiovascular disease. Nat. Rev. Cardiol.20, 600–616 (2023). - PubMed
-
- Cardiovascular disease: risk assessment and reduction, including lipid modification. London: National Institute for Health and Care Excellence (NICE) (2023). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
