

Epidemiological study of hospital acquired acute kidney injury in critically ill and its effect on the survival
- PMID: 39548198
- PMCID: PMC11568283
- DOI: 10.1038/s41598-024-79533-6
Epidemiological study of hospital acquired acute kidney injury in critically ill and its effect on the survival
Abstract
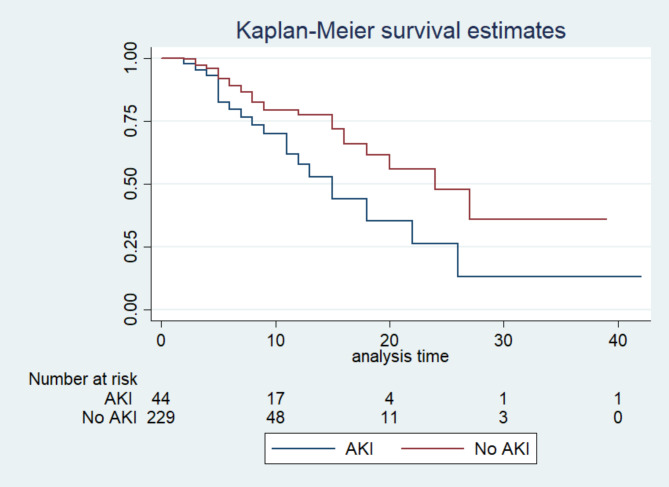
In the intensive care unit (ICU), acute kidney injury (AKI) is the most common cause of morbidity and mortality. Hospital-acquired acute kidney injury (HAAKI) is AKI developing after 48 h. We aimed to study the development of AKI and its associated risk factors. We conducted a longitudinal observational study. Inclusion criteria were patients > 18 years of age admitted to ICU. The primary outcome was the development of AKI as defined by Kidney Disease Improving Global Outcomes (KDIGO) criteria. A total of 273 patients were included in the study. Out of 273, 44(16.11%) patients developed AKI. The mean age was 45.80(17.39) years, and 60.81% were males. The median acute physiology and chronic health evaluation (APACHE II) and sequential organ failure assessment (SOFA) scores were 12(8-18) and 5(3-7), respectively. Diabetes mellitus (23.44%) and hypertension (23.81%) were predominant comorbidities. The risk factors associated with AKI were serum chloride level, colistin, invasive ventilation, positive end-expiratory pressure (PEEP), and fluid balance. The hospital mortality was significantly higher in patients with AKI (43.18%) as compared with no AKI (14.41%). Among the secondary outcomes, 7 (15.90%) patients required renal replacement therapy (RRT) during hospitalisation. The length of ICU stay was higher in patients with AKI 8(5-13) compared to no AKI 5(3-8). A total of 16.11% developed HAAKI, and mortality was 43.18%. Post 6 months follow-up of AKI patients, mortality was 23%. Among survivors none of the patients were on RRT.Patients admitted with normal kidney function can develop AKI. Hence, careful monitoring of ICU patients is necessary.
Keywords: Acute Kidney Injury; Critically ill; HAAKI; KDIGO; Renal Replacement Therapy; Sepsis.
© 2024. The Author(s).
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
