

Persistence diagrams for exploring the shape variability of abdominal aortic aneurysms
- PMID: 39548199
- PMCID: PMC11568180
- DOI: 10.1038/s41598-024-78301-w
Persistence diagrams for exploring the shape variability of abdominal aortic aneurysms
Abstract
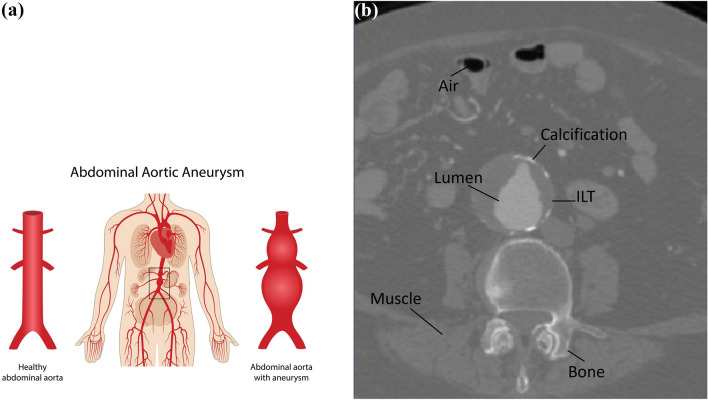
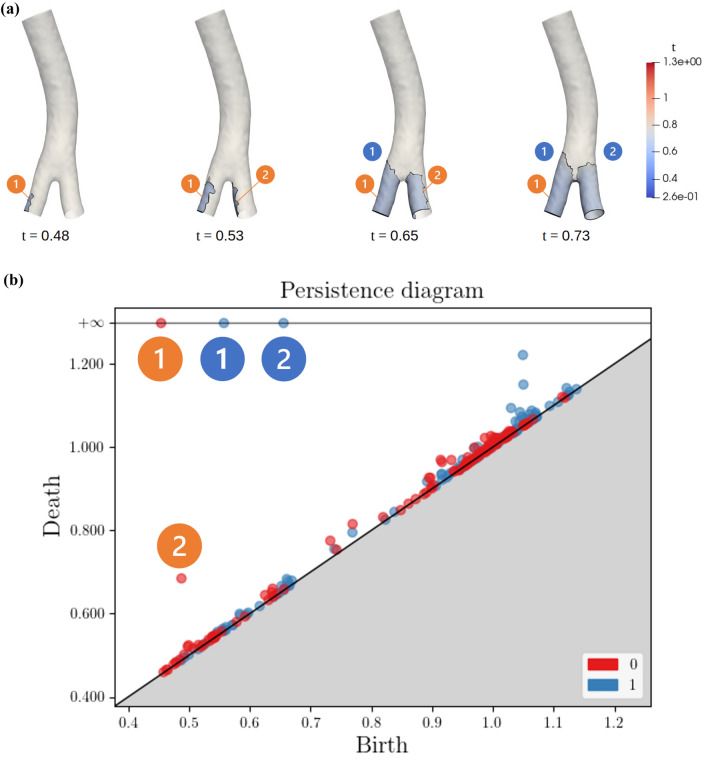
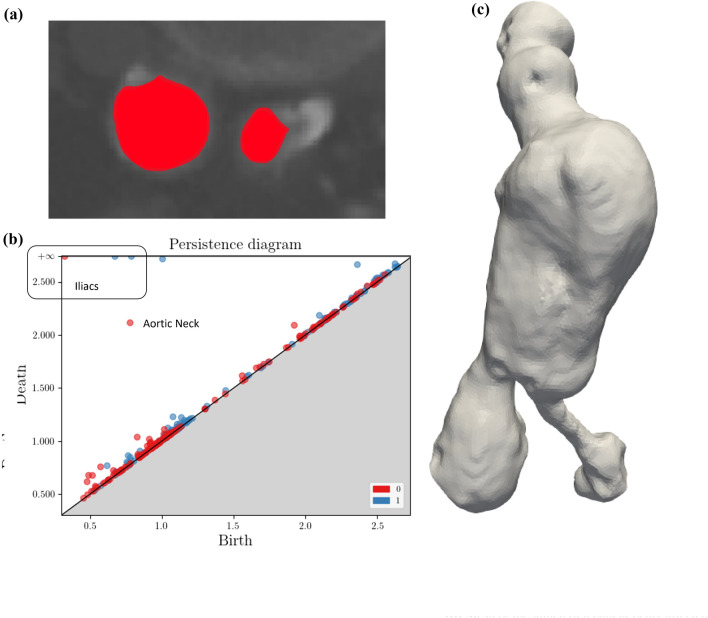
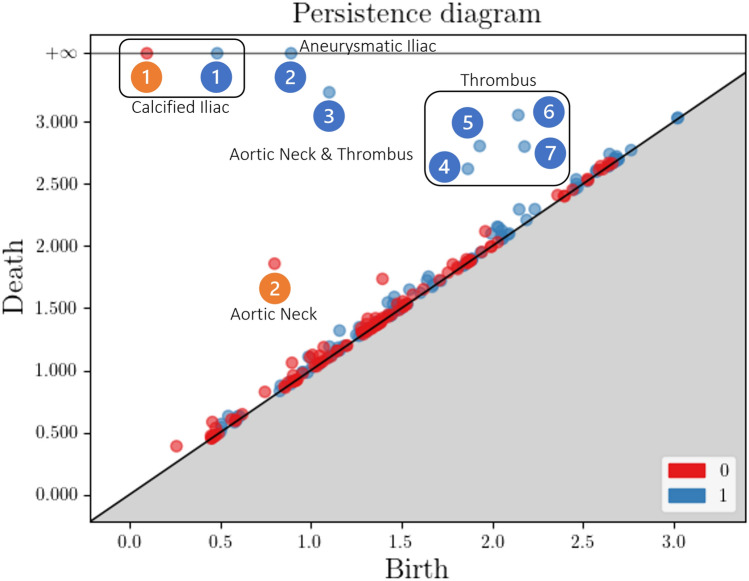
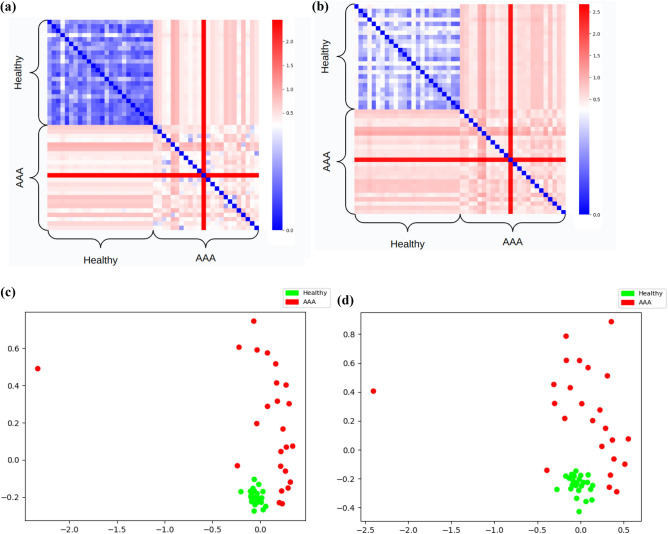
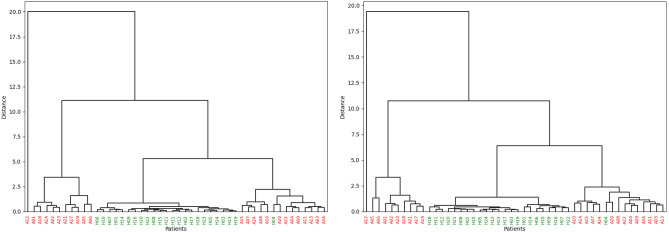
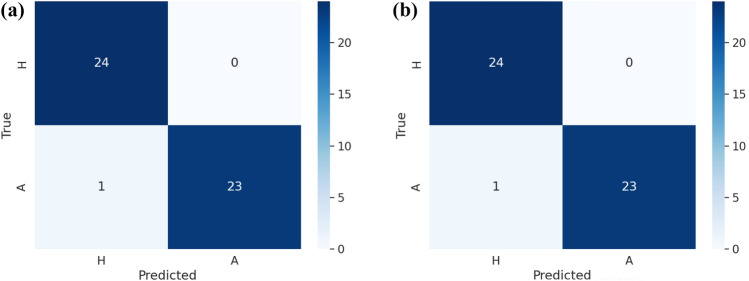
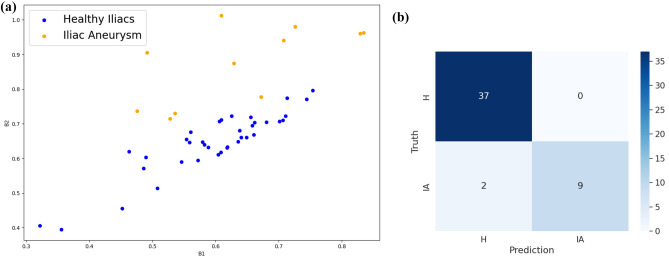
Abdominal aortic aneurysm consists of a permanent dilation in the abdominal portion of the aorta and, along with its associated pathologies like calcifications and intraluminal thrombi, is one of the most important pathologies of the circulatory system. The shape of the aorta is among the primary drivers for these health issues, with particular reference to all the characteristics which affect the hemodynamics. Starting from the computed tomography angiography of a patient, we propose to summarize such information using tools derived from Topological Data Analysis, obtaining persistence diagrams which describe the irregularities of the lumen of the aorta. We showcase the effectiveness of such shape-related descriptors with a series of supervised and unsupervised case studies.
© 2024. The Author(s).
Conflict of interest statement
Figures











References
-
- Marron, J. S. & Dryden, I. L. Object Oriented Data Analysis (CRC Press, 2021).
-
- Sonesson, B., Länne, T., Hansen, F. & Sandgren, T. Infrarenal aortic diameter in the healthy person. Eur. J. Vasc. Endovasc. Surg.8, 89–95 (1994). - PubMed
-
- Wilson, K. A., Lindholt, J. S., Hoskins, P. R. & et al. The relationship between abdominal aortic aneurysm distensibility and serum markers of elastin and collagen metabolism. Eur. J. Vasc. Endovasc. Surg.21, 175–178 (2001). - PubMed
-
- Mealy, K. & Salman, A. The true incidence of ruptured abdominal aortic aneurysms. Med. Eng. Phys2, 405–408 (1988). - PubMed
