

Sirtuin inhibitors reduce intracellular growth of M. tuberculosis in human macrophages via modulation of host cell immunity
- PMID: 39548210
- PMCID: PMC11568201
- DOI: 10.1038/s41598-024-79136-1
Sirtuin inhibitors reduce intracellular growth of M. tuberculosis in human macrophages via modulation of host cell immunity
Abstract
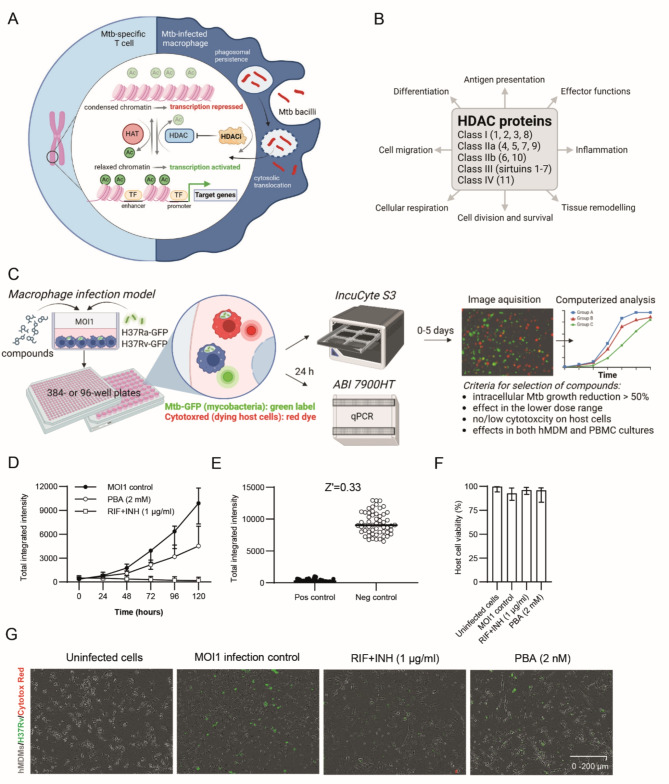
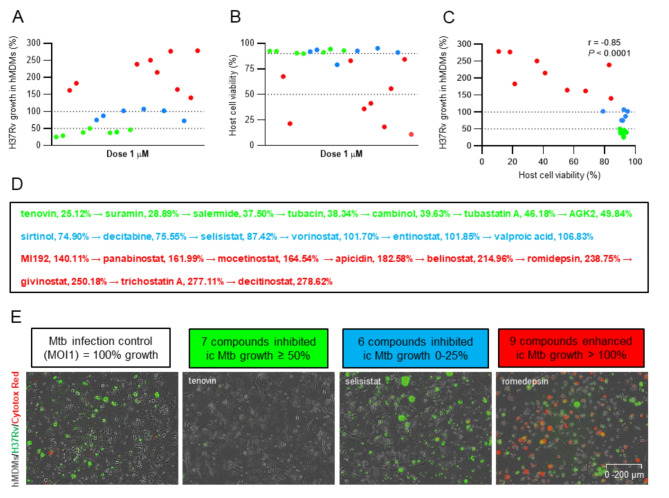
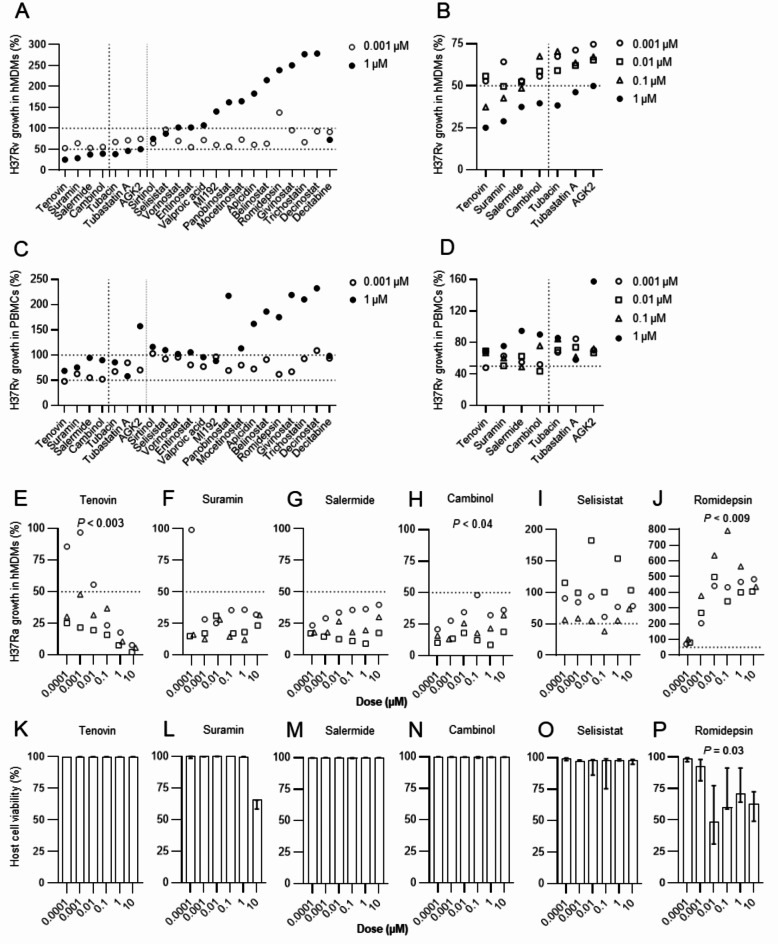
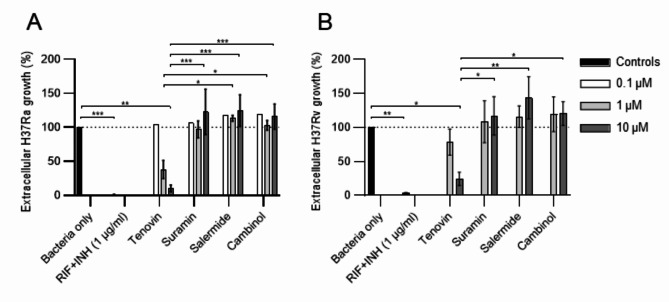
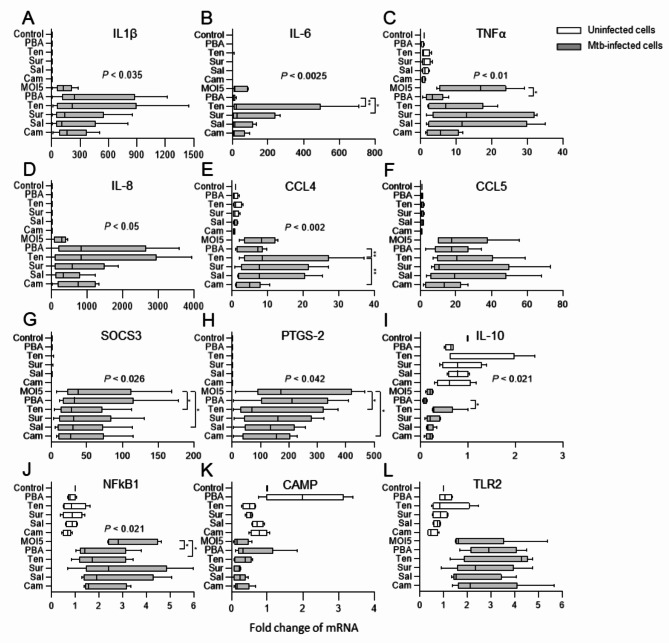
Host-directed therapies aiming to strengthen the body's immune system, represent an underexplored opportunity to improve treatment of tuberculosis (TB). We have previously shown in Mycobacterium tuberculosis (Mtb)-infection models and clinical trials that treatment with the histone deacetylase (HDAC) inhibitor, phenylbutyrate (PBA), can restore Mtb-induced impairment of antimicrobial responses and improve clinical outcomes in pulmonary TB. In this study, we evaluated the efficacy of different groups of HDAC inhibitors to reduce Mtb growth in human immune cells. A panel of 21 selected HDAC inhibitors with different specificities that are known to modulate infection or inflammation was tested using high-content live-cell imaging and analysis. Monocyte-derived macrophages or bulk peripheral blood cells (PBMCs) were infected with the green fluorescent protein (GFP)-expressing Mtb strains H37Ra or H37Rv and treated with HDAC inhibitors in the micromolar range in parallel with a combination of the first-line antibiotics, rifampicin, and isoniazid. Host cell viability in HDAC inhibitor treated cell cultures was monitored with Cytotox-red. Seven HDAC inhibitors were identified that reduced Mtb growth in macrophages > 45-75% compared to average 40% for PBA. The most effective compounds were inhibitors of the class III HDAC proteins, the sirtuins. While these compounds may exhibit their effects by improving macrophage function, one of the sirtuin inhibitors, tenovin, was also highly effective in extracellular killing of Mtb bacilli. Antimicrobial synergy testing using checkerboard assays revealed additive effects between selected sirtuin inhibitors and subinhibitory concentrations of rifampicin or isoniazid. A customized macrophage RNA array including 23 genes associated with cytokines, chemokines and inflammation, suggested that Mtb-infected macrophages are differentially modulated by the sirtuin inhibitors as compared to PBA. Altogether, these results demonstrated that sirtuin inhibitors may be further explored as promising host-directed compounds to support immune functions and reduce intracellular growth of Mtb in human cells.
Keywords: Mycobacterium tuberculosis; Histone deacetylase (HDAC) inhibitors; Host-directed therapy; Immunity; Macrophage; Sirtuins; Tuberculosis.
© 2024. The Author(s).
Conflict of interest statement
Figures


References
-
- Barilar, I. et al. Emergence of bedaquiline-resistant tuberculosis and of multidrug-resistant and extensively drug-resistant Mycobacterium tuberculosis strains with rpoB Ile491Phe mutation not detected by Xpert MTB/RIF in Mozambique: a retrospective observational study. Lancet Infect. Dis.24, 297–307. 10.1016/S1473-3099(23)00498-X (2024). - PubMed
-
- Rao, M. et al. Improving treatment outcomes for MDR-TB - Novel host-directed therapies and personalised medicine of the future. Int. J. Infect. Dis.80S, S62–S67. 10.1016/j.ijid.2019.01.039 (2019). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
