

Different antithrombotic strategies to prevent cardiovascular complications in Kawasaki patients: a systematic review and meta-analysis
- PMID: 39548432
- PMCID: PMC11566157
- DOI: 10.1186/s12887-024-05202-2
Different antithrombotic strategies to prevent cardiovascular complications in Kawasaki patients: a systematic review and meta-analysis
Abstract
Background: Coronary artery aneurysm (CAA) poses significant cardiovascular risks, particularly in Kawasaki disease (KD) patients. This systematic review and meta-analysis aim to evaluate and compare antithrombotic strategies in preventing CAA formation secondary to Kawasaki disease and the ensuing CAA cardiovascular complications.
Methods: Following PRISMA guidelines, we systematically searched major databases, namely PubMed, Scopus, Web of Science, and Embase. Major adverse cardiovascular events (MACE), myocardial infarction (MI), stenosis, bleeding, occlusion, and coronary artery lesion (CAL) formation were primary outcomes. Consolidated Standards of Reporting Trials (CONSORT) and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) scores assessed study quality. A meta-analysis, as well as sensitivity analysis and meta-regression, was performed to compare the efficacy of pharmacological strategies on the outcomes.
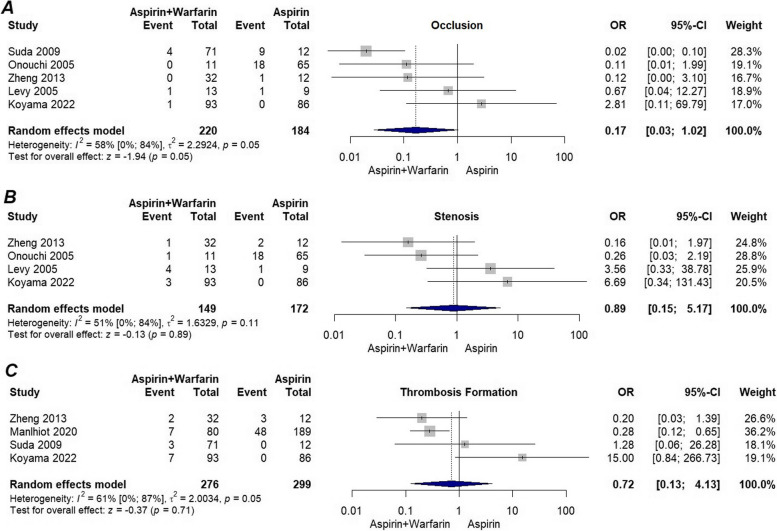
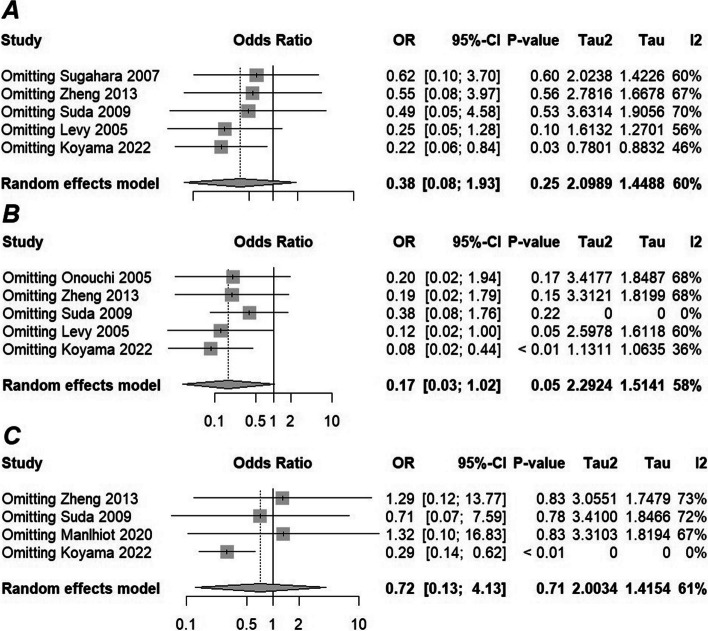
Results: The study included 21 studies with 1045 patients for CAA complications and 41536 patients for CAA formation prevention. In children with CAA secondary to Kawasaki disease, the addition of warfarin to aspirin was associated with a significantly lower odds of myocardial infarction (OR = 0.26, 95% CI: 0.11-0.60, I2 = 25%) and mortality (OR = 0.18, 95% CI: 0.04-0.88, I2 = 0%) compared to aspirin alone. However, there was no significant difference in MACE (OR = 0.38, 95% CI: 0.08-1.93, I2 = 60%) and occlusion (OR = 0.17, 95% CI: 0.02-1.92, I2 = 58%). Sensitivity analysis showed reduced thrombosis (OR = 0.29, 95% CI: 0.14-0.62, I2 = 0%), MACE (OR [95% CI] = 0.22[0.06-0.84], I2 = 46%), and occlusion (OR [95% CI] = 0.08[0.02-0.44], I2 = 36%). Meta-regression did not yield significant results.
Conclusions: As for the acute phase of KD, no benefit was conferred from adding high-dose aspirin to the routine IVIG alone regimen. However, the complexity of outcomes and the diversity in antithrombotic interventions underscore the need for tailored approaches and further research.
Keywords: Cardiovascular Complications; Kawasaki disease; Meta-analysis; Prevention; Systematic Review.
© 2024. The Author(s).
Conflict of interest statement
Figures




Similar articles
-
Safety and efficacy of warfarin plus aspirin combination therapy for giant coronary artery aneurysm secondary to Kawasaki disease: a meta-analysis.Cardiology. 2014;129(1):55-64. doi: 10.1159/000363732. Epub 2014 Aug 12. Cardiology. 2014. PMID: 25116427 Review.
-
Coronary Artery Aneurysms in Kawasaki Disease: Risk Factors for Progressive Disease and Adverse Cardiac Events in the US Population.J Am Heart Assoc. 2016 Sep 15;5(9):e003289. doi: 10.1161/JAHA.116.003289. J Am Heart Assoc. 2016. PMID: 27633390 Free PMC article.
-
Low-dose antithrombotic treatment in coronary thrombosis of Kawasaki disease.Pediatr Cardiol. 2015 Mar;36(3):503-8. doi: 10.1007/s00246-014-1040-1. Epub 2014 Oct 9. Pediatr Cardiol. 2015. PMID: 25298222
-
Pharmacologic interventions for Kawasaki disease in children: A network meta-analysis of 56 randomized controlled trials.EBioMedicine. 2022 Apr;78:103946. doi: 10.1016/j.ebiom.2022.103946. Epub 2022 Mar 17. EBioMedicine. 2022. PMID: 35306339 Free PMC article.
-
[Secondary prevention after acute myocardial infarction: aspirin, warfarin or both?].Tidsskr Nor Laegeforen. 2003 Jun 26;123(13-14):1838-40. Tidsskr Nor Laegeforen. 2003. PMID: 12830258 Review. Norwegian.
Cited by
-
Antithrombotic therapy in adults with ectatic coronary artery disease: a systematic review and network meta-analysis.Egypt Heart J. 2025 Jan 22;77(1):13. doi: 10.1186/s43044-025-00612-8. Egypt Heart J. 2025. PMID: 39841407 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
