

Emergency neurosurgery for traumatic brain injury by general surgeons at local hospitals in Sweden: a viable option when time is brain
- PMID: 39548552
- PMCID: PMC11568597
- DOI: 10.1186/s13049-024-01290-2
Emergency neurosurgery for traumatic brain injury by general surgeons at local hospitals in Sweden: a viable option when time is brain
Abstract
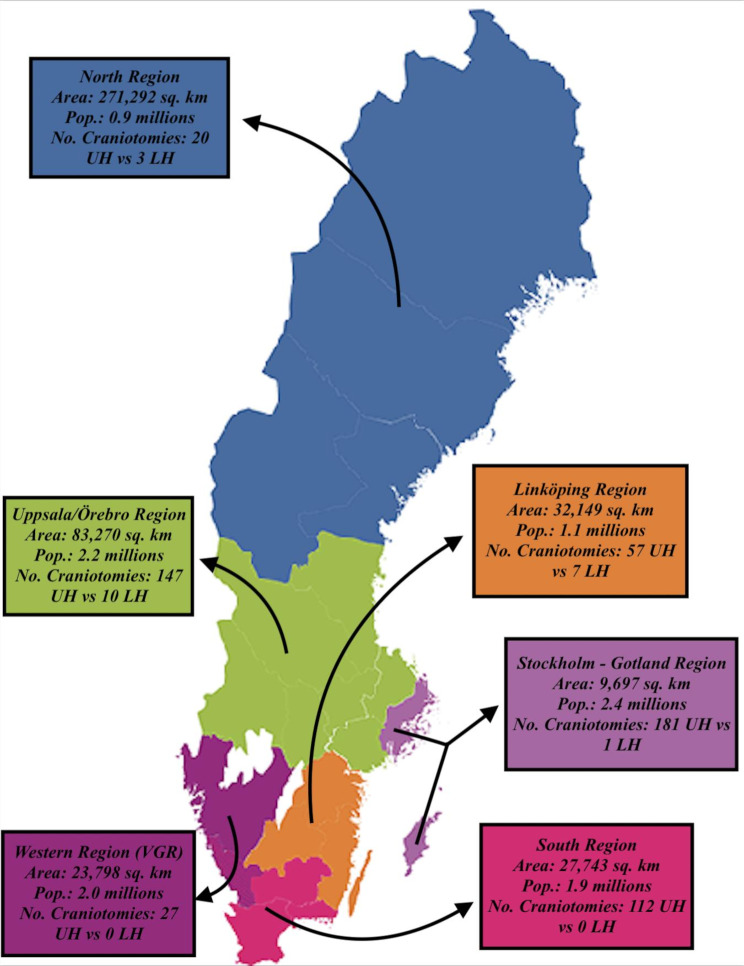
Background: Timing of surgical evacuation of mass lesions in traumatic brain injury (TBI) is crucial. However, due to geographical variations, transportation time to the nearest neurosurgical department may be long. To save time, general surgeons at a local hospital may perform the operation, despite more limited experience in neurosurgical techniques. This study aimed to determine whether patient outcomes differed between those who had undergone emergency neurosurgery at local hospitals by general surgeons vs. at university hospitals by neurosurgeons.
Methods: A nationwide observational study was performed using data from the Swedish Trauma Registry (SweTrau) between 2018 and 2022. A total of 565 TBI patients (local hospitals, n = 21; university hospitals, n = 544) who underwent intracranial hematoma evacuation within 8 h after arrival at the hospital were included. Data on demography, admission variables, traumatic injuries, and outcome (Glasgow Outcome Scale [GOS]) at discharge were evaluated. Favourable vs. unfavourable outcomes were defined as GOS scores of 4-5 vs. 1-3.
Results: Compared with those treated at university hospitals, patients treated with intracranial hematoma evacuation at local hospitals had lower median Glasgow Coma Scale (GCS) scores (8 vs. 12, p < 0.001), higher rate of acute subdural hematomas (86% vs. 77%, p < 0.001), and lower rate of contusions (14% vs. 53%, p = 0.01). Being operated on at a local hospital was independently associated with higher mortality (p = 0.03) but with a similar rate of favourable outcome (p = 0.74) in multiple logistic regressions after adjustment for demographic and injury-related variables.
Conclusions: Although a slightly greater proportion of patients who underwent emergency neurosurgery at local hospitals died, there was no difference in the rate of favourable outcome. Thus, in patients with impending brain herniation, when time is of the essence, evacuation of traumatic intracranial bleeding by general surgeons at local hospitals remains a highly viable option.
Keywords: Craniotomy; Intracranial bleeding; Neurosurgery; Outcome; Traumatic brain injury.
© 2024. The Author(s).
Conflict of interest statement
Figures


Similar articles
-
Temporal delays in trauma craniotomies.J Neurosurg. 2016 Sep;125(3):642-7. doi: 10.3171/2015.6.JNS15175. Epub 2016 Jan 1. J Neurosurg. 2016. PMID: 26722857
-
Nonsurgical acute traumatic subdural hematoma: what is the risk?J Neurosurg. 2015 Nov;123(5):1176-83. doi: 10.3171/2014.10.JNS141728. Epub 2015 May 8. J Neurosurg. 2015. PMID: 25955872
-
Acute neurosurgery for traumatic brain injury by general surgeons in Swedish county hospitals: a regional study.Acta Neurochir (Wien). 2014 Jan;156(1):177-85. doi: 10.1007/s00701-013-1932-5. Epub 2013 Nov 24. Acta Neurochir (Wien). 2014. PMID: 24272412
-
Prognostic Significance of Magnetic Resonance Imaging in Detecting Diffuse Axonal Injuries: Analysis of Outcomes and Review of Literature.Neurol India. 2022 Nov-Dec;70(6):2371-2377. doi: 10.4103/0028-3886.364066. Neurol India. 2022. PMID: 36537418 Review.
-
Decision making in very severe traumatic brain injury (Glasgow Coma Scale 3-5): a literature review of acute neurosurgical management.J Neurosurg Sci. 2018 Apr;62(2):153-177. doi: 10.23736/S0390-5616.17.04255-2. Epub 2017 Nov 10. J Neurosurg Sci. 2018. PMID: 29125266 Review.
Cited by
-
Regional variation in traumatic brain injury patterns, management and mortality: a nationwide Swedish cohort study.Acta Neurochir (Wien). 2025 May 8;167(1):134. doi: 10.1007/s00701-025-06557-w. Acta Neurochir (Wien). 2025. PMID: 40338360 Free PMC article.
References
-
- Dewan MC, Rattani A, Gupta S, Baticulon RE, Hung YC, Punchak M, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2018;130(4):1080–97. - PubMed
-
- Wang HK, Lin SH, Sung PS, Wu MH, Hung KW, Wang LC, et al. Population based study on patients with traumatic brain injury suggests increased risk of dementia. J Neurol Neurosurg Psychiatry. 2012;83(11):1080–5. - PubMed
-
- Skoglund TS, Nellgård B. Long-time outcome after transient transtentorial herniation in patients with traumatic brain injury. Acta Anaesthesiol Scand. 2005;49(3):337–40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
